|
I have listed references
here to some studies that demonstrate positive and negative
health effects of three other common water contaminants.
These are just a few of the papers that you can find during
a brief search of PubMed that can support drastically different
conclusions about the health effects of these contaminants
- take a look.
|
|
The
National Library
of Medicine makes medical and scientific journal abstracts and some
entire articles available to the general public. Most journals represented
publish peer-reviewed studies for much of the medical and scientific research
world wide.
Below are some examples of research papers from the
1950s into 2015 on fluoride and fluoridation to counter
the argument that there is NO recent evidence that water fluoridation is
beneficial or safe. As mentioned elsewhere, there are also
a few studies listed which examine possible risks.
I discuss elsewhere
details of the many concerns I have with the way fluoridation opponents
present their evidence, but I included a
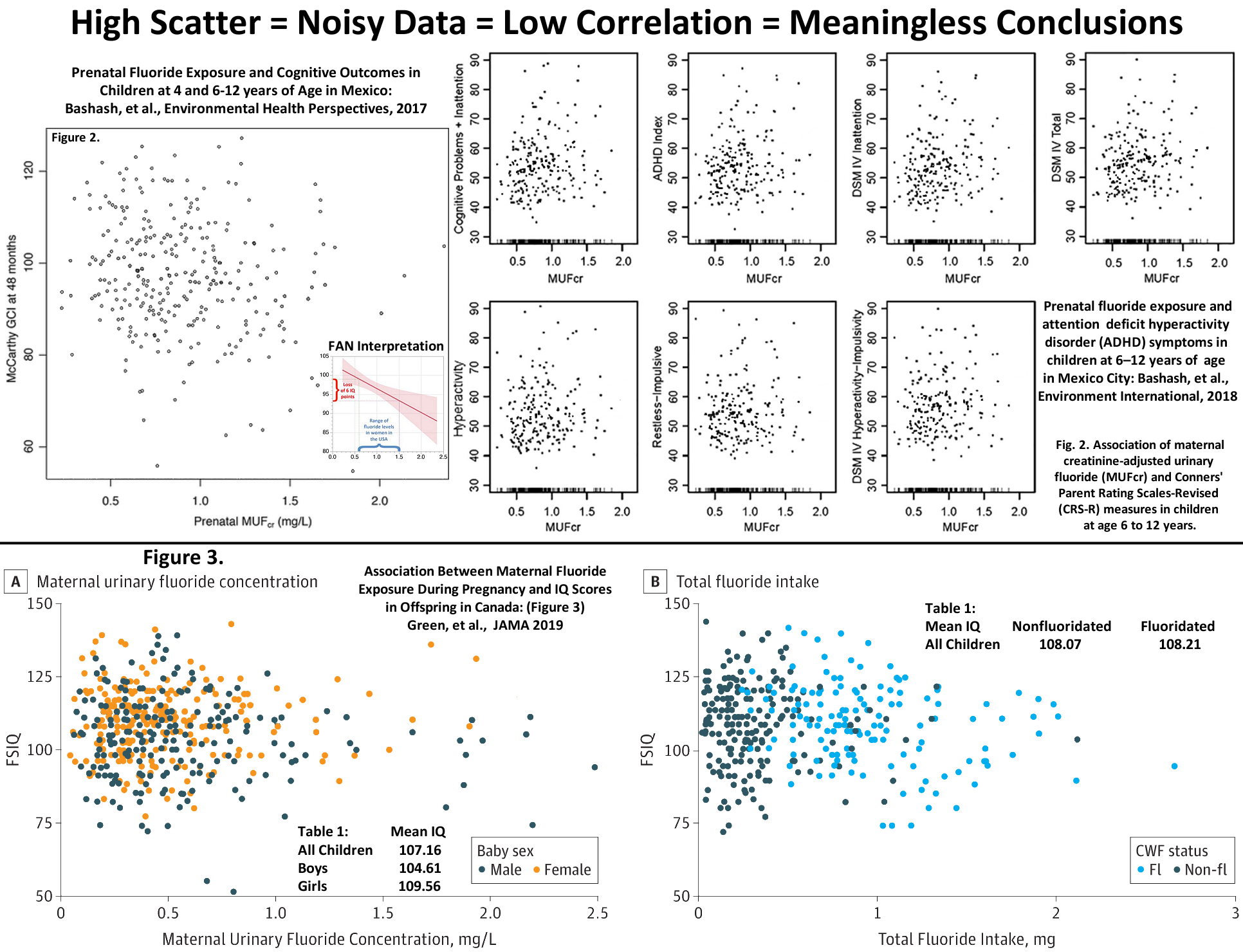
specific example (Evidence? tab) that contrasts two published studies to illustrate the differences
between a paper that presents evidence that fluoridation does not have a
negative effect on IQ and another paper used by fluoride opponents to bolster
their claim that fluoridation decreases IQ.
I encourage you to evaluate for yourself the evidence for and
against community drinking water fluoridation (CWF) with an
open mind. If you are not a scientist, and/or if you have strong
existing beliefs one way or another, that is an extremely daunting task.
Fluoridation, like other scientific topics, is very complex, the studies
are not easy to understand, and you can find studies that apparently
support either side. Compare the content and conclusions of
these recent reviews and studies (and those cited below) that
accurately highlight the benefits and risks of CWF with the way studies
are presented by fluoridation opponents who frequently exaggerate and.or
misrepresent study conclusions and cite studies that have nothing to do
with drinking optimally fluoridated water.
search the National Library of Medicine and
Search www.ncbi.nlm.nih.gov/pubmed
for terms related to water fluoridation. A search on general topics
like, fluoridation will return a large number of results (6,609 in
January 2020), or community water fluoridation, (1,147 results), but it is a
good way to find other words to include that limit the search. For
example you can reduce the number of results to a more manageable size by
using more restrictive search terms like: water fluoridation caries
(3,409 results); water fluoridation safety (137 results); water
fluoridation benefits (226 results); water fluoridation risks
(599 results); drinking water fluoridation (970 results);
fluoridation health (2,755 results); water fluoridation cancer
(169 results - note that virtually none of the papers actually study the
link between fluoridation and cancer); water fluoridation brain (15
results - note the 2010 paper on fluoride-induced oxidative stress in the rat
brain used concentrations of fluoride in the water 100-200 times greater
than found in fluoridated water); water fluoridation IQ (1 result); water
fluoridation fractures (90 results); fluoridation ethics (62
results); fluoridation cost (429 results). If you take time
to look through the medical literature on any aspect of fluoridation, I
am confident you will discover that papers which support the effectiveness
and safety of fluoridation significantly outnumber those which report risks of fluoridation
(at recommended levels). If you understand how
scientific studies are designed and conducted - and the results analyzed
and reported - you will also see the limitations of most studies that
report harm from or ineffectiveness of community water fluoridation.
Fluoridation opponents list on their websites many papers which document
claims that fluoridation is harmful and not effective. Many of these
papers are not archived at the National Library of Medicine. This
typically means the papers have not been published in recognized peer-reviewed
journals. The reason usually given is that the traditional dental,
medical and scientific communities are so committed to community water fluoridation
that they actively block funding and publication of any research that might
uncover health risks of fluoridation. There is, of course another
explanation: The majority of research that shows other health risks at optimal
fluoridation besides the risks of dental fluorosis, is simply not of high
enough quality to be published in a peer reviewed journal. The publication,
Fluoridation Facts, produced by the American Dental Association,
describes some of the conditions under which conclusions reached by a study
might not be acceptable for publication.
Below is a sample of about 220 research papers and reviews that should, without any question,
dispel the myth propagated by some fluoridation opponents that there is
no current evidence to support the safety and effectiveness of drinking water
fluoridation. This evidence (updated 10/3/2018) provides specific
citations and conclusions from over 60 years of research (1950 - 2018).
Community Water Fluoridation Programs:
A Health Technology Assessment — Review of Dental Caries and Other Health Outcomes The evidence in this review supports the protective effect of CWF in reducing dental caries
in both deciduous and permanent teeth in children and in permanent teeth in adults, despite
the widespread availability and use of fluoridated toothpaste in the current settings. Dental fluorosis prevalence may increase with increasing water fluoride levels,
but dental fluorosis of “aesthetic concern” among Canadian children is rare. There was
evidence that there may be no association between water fluoridation at the current
Canadian levels and bone cancer, total cancer incidence, hip fracture, Down syndrome, and
IQ and cognitive function. (p 227) (Canadian Agency for Drugs and Technologies in Health; Feb.
2019)
Community Water Fluoridation Exposure:
A Review of Neurological and Cognitive Effects
The aim of this report is to review recent evidence
[specifically, the 2019 Green, et al. study] on the effects of fluoride exposure through CWF at levels that are relevant to the Canadian context on the neurological or cognitive development in children and adolescents less than 18 years of age. The findings reported by the
[Green, et al.] study in this review provided weak evidence and should be interpreted carefully, given the multiple aforementioned limitations. This, along with other evidence described in the CADTH Review of Dental Caries and Other Health Outcomes on CWF
[referenced above] which demonstrated no association with IQ and cognitive function should be considered. Canadian Agency for Drugs and Technologies in Health; 2019 Oct 23.)
https://ww.ncbi.nlm.nih.gov/pubmed/29404855
National Toxicity Program fluoride study, An Evaluation of Neurotoxicity Following Fluoride Exposure from Gestational Through Adult Ages in Long-Evans Hooded Rats: At these exposure levels, we observed no exposure-related differences in motor, sensory, or learning and memory performance on running wheel, open-field activity, light/dark place preference, elevated plus maze, pre-pulse startle inhibition, passive avoidance, hot-plate latency, Morris water maze acquisition, probe test, reversal learning, and Y-maze. T3, T4, and TSH levels were not altered as a function of 10 or 20 ppm F- in the drinking water. No exposure-related pathology was observed in the heart, liver, kidney, testes, seminal vesicles, or epididymides. Mild inflammation in the prostate gland was observed at 20 ppm F-. No evidence of neuronal death or glial activation was observed in the hippocampus at 20 ppm F-. (McPherson, et al., Neurotox Res. 2018)
https://www.ncbi.nlm.nih.gov/pubmed/30213354
The Role of Fluoride in the Prevention of Tooth Decay: Although there are recommendations to prevent tooth decay by other means, this nonsystematic review finds that fluoride is the key to prevention and control of tooth decay. There are multiple fluoride modalities with effectiveness and safety of fluoride depending on dose and concentration. Prevention of tooth decay occurs at the individual level by fluoride use at home and with professional application and at the community level through fluoridation of water or salt. (Pollick H, Pediatr Clin North Am. 2018)
https://www.ncbi.nlm.nih.gov/pubmed/28648551
Science, Politics, and Communication: The Case of Community Water Fluoridation in the US: Community water fluoridation (CWF) and its effect in reducing the burden of dental caries (tooth decay) is considered one of the 10 public health achievements in the 20th century. In the U.S., three-quarters (74.4%) of people on community water supplies have optimally fluoridated water, and each year approximately 90 communities actively consider starting or discontinuing CWF.
... The continued involvement of epidemiologists as part of multidisciplinary teams is needed in research, surveillance, peer review of studies, assessment of systematic review findings, and in the translation and communication of science findings to audiences with limited science/health literacy. (Allukian M Jr, et al., Ann Epidemiol. 2018)
https://www.ncbi.nlm.nih.gov/pubmed/30188616
A multi-variable analysis of four factors affecting caries levels among five-year-old children; deprivation, ethnicity, exposure to fluoridated water and geographic region: CONCLUSIONS: Five-year-old children who were from the most deprived areas, not exposed to fluoridated water, of an Eastern European ethnic group and living in the North West demonstrated the highest prevalence and severity of caries in the survey under scrutiny. This is of public health importance, providing evidence for population groups to target with health improvement activities. (Weston-Price, et al., Community Dent Health. 2018)
https://www.ncbi.nlm.nih.gov/pubmed/30109528
Fluoridation and county-level secondary bone cancer among cancer patients 18 years or older in New York State: We found no evidence of an association between community water fluoridation category and secondary bone cancer from 2008 to 2010 at the county level in New York State. (Crnosija, et al., Environ Geochem Health. 2018)
https://www.ncbi.nlm.nih.gov/pubmed/29900806
Water Fluoridation and Dental Caries in U.S. Children and Adolescents:
These findings confirm a substantial caries-preventive benefit of CWF for U.S. children and that the benefit is most pronounced in primary teeth. (Slade, et al., J Dent Res. 2018)
Interview with Dr. Slade.
https://www.ncbi.nlm.nih.gov/pubmed/29869803
Contemporary evidence on the effectiveness of water fluoridation in the prevention of childhood caries: CONCLUSION: Analysis of contemporary data representative of the Australian child population found consistent associations between %LEFW and childhood caries, which persisted when socioeconomic differences were adjusted across exposure groups, supporting the continued effectiveness of water fluoridation. (Spencer, et al., Community Dent Oral Epidemiol. 2018)
https://www.ncbi.nlm.nih.gov/pubmed/29641653
Caries and fluoridated water in two Brazilian municipalities with low prevalence of the disease: CONCLUSIONS: Exposure to fluoridated water implied lower mean values for the DMFT and SiC indexes, even in the presence of the concomitant exposure to fluoridated toothpaste, in a scenario of low prevalence of the disease, and with a similar pattern of caries distribution in the populations analyzed. (Cruz & Narvai, Rev Saude Publica. 2018)
https://www.ncbi.nlm.nih.gov/pubmed/29192688
Fluoridation and attention deficit hyperactivity disorder - a critique of Malin and Till (2015): A recent ecological study found a statistically significant association of attention deficit hyperactivity disorder (ADHD) prevalence in youth with exposure to fluoride in fluoridated water. However, it included only household income as a possible covariate. In contrast another study found a significant association of ADHD prevalence with residential altitude. A multiple regression analysis including water fluoridation extent, mean US state elevation and a number of possibly important social factors as covariates showed statistically significant associations of ADHD prevalence in 2011 with altitude and per capita personal income in 2009. There was no statistically significant association of ADHD with the exposure to fluoride when these covariates were included. The ADHD-fluoridation study suffers from insufficient consideration of possible risk-modifying factors but has been widely cited because its reported findings appear advantageous to political campaigns against community water fluoridation. (Perrott, K, Br Dent J. 2018)
https://www.ncbi.nlm.nih.gov/pubmed/29179712
Full Article
The costs and benefits of water fluoridation in NZ: RESULTS: Over 20 years, the net discounted saving from adding fluoride to reticulated water supplies supplying populations over 500 would be NZ$1401 million, a nine times pay-off. Between 8800 and 13,700 quality-adjusted life years would be gained. While fluoridating reticulated water supplies for large communities is cost-effective, it is unlikely to be so with populations smaller than 500. CONCLUSIONS:
Community water fluoridation remains highly cost-effective for all but very small communities. The health benefits-while (on average) small per person-add up to a substantial reduction in the national disease burden across all ethnic and socioeconomic groups. (Moore, et al., BMC Oral Health. 2017)
https://www.ncbi.nlm.nih.gov/pubmed/29072650
Caries prevention with fluoridated and iodinated salt in school-aged children living in areas with fluoride and iodine deficiency:
The aim of the study was to evaluate the efficacy of dental caries prevention program with 3 years follow-up in children living in areas with fluoride and iodine deficiency. The study involved 625 school-aged children aged 6, 12 and 15 years receiving endogenous prevention with fluoridated and iodinated salt (300±50 mgF/kg and 40±10 mgI/kg). Obtained reduction of DMFT growth, positive changes of mineral composition and dental hard tissues microhardness prove high clinical efficacy of applied prevention program. (Ahmedbeyli RM, Stomatologiia (Mosk). 2017)
https://ww.ncbi.nlm.nih.gov/pubmed/29171664:
Does water fluoridation affect the prevalence of enamel fluorosis differently among racial and ethnic groups? CONCLUSIONS: Enamel fluorosis was not associated with race/ethnicity. Our analysis suggests that exposure to similar levels of fluoride in the water does not appear to place certain race/ethnic groups at a higher risk for developing enamel fluorosis, and lowering the optimal range of drinking water fluoride to a single value of 0.7 ppm will provide a level of protection against enamel fluorosis that will benefit all race/ethnicity groups. (Arora, et al., J Public Health Dent. 2018)
https://www.ncbi.nlm.nih.gov/pubmed/28910243
Fluoride exposure and reported learning disability diagnosis among Canadian children: Implications for community water fluoridation: CONCLUSION: Overall, there did not appear to be a robust association between fluoride exposure and parental- or self-reported diagnosis of a learning disability among Canadian children. (Barberio, et al., Can J Public Health. 2017)
https://www.ncbi.nlm.nih.gov/pubmed/28839078
Full Article
Fluoride exposure and indicators of thyroid functioning in the Canadian population: implications for community water fluoridation: RESULTS: There was no evidence of a relationship between fluoride exposure (from urine and tap water) and the diagnosis of a thyroid condition. There was no statistically significant association between fluoride exposure and abnormal (low or high) TSH levels relative to normal TSH levels. CONCLUSION: These analyses suggest that, at the population level, fluoride exposure is not associated with impaired thyroid functioning in a time and place where multiple sources of fluoride exposure, including CWF, exist. (Barberio, et al., J Epidemiol Community Health. 2017)
https://www.ncbi.nlm.nih.gov/pubmed/28808691
Full Article
Fluoride Depletes Acidogenic Taxa in Oral but Not Gut Microbial Communities in Mice: [F]luoride treatment did not induce a significant shift in gut microbial community composition or function in our mouse model, possibly due to absorption in the upper gastrointestinal tract. Fluoride-associated perturbations thus appeared to have a selective effect on the composition of the oral but not gut microbial community in mice. (Yasuda, et al., mSystems. 2017)
https://www.ncbi.nlm.nih.gov/pubmed/28737337
Salt fluoridation and dental caries: state of the question: RESULTS:
After a literature search, 22 references were selected reporting data on the preventive effect of salt fluoridation programmes in Europe (Hungary, Switzerland, France, Germany) and South and Central America (Colombia, Mexico, Jamaica...). Data were mainly obtained from descriptive or retrospective epidemiological studies. The results indicate that, in the absence of topical fluoride support, salt fluoridation leads to a significant reduction in caries indexes among treated children compared to a control group. (Vautey, et al., Sante Publique. 2017)
https://www.ncbi.nlm.nih.gov/pubmed/28404475
CONCLUSIONS: Exploring the short-term impact of community water fluoridation cessation on children's dental caries: a natural experiment in Alberta, Canada:
Our results suggest an increase in dental caries in primary teeth during a time period when community fluoridation was ceased. That we did not observe a worsening for permanent teeth in the comparative analysis could reflect the limited time since cessation. It is imperative that efforts to monitor these trends continue. (McLaren, et al., Public Health. 2017)
https://www.ncbi.nlm.nih.gov/pubmed/28243675
Full Article
Communicating about risk: strategies for situations where public concern is high but the risk is low: In this article, we summarise research that identifies best practice for communicating about hazards where the risk is low but public concern is high. We apply Peter Sandman's 'risk = hazard + outrage' formulation to these risks, and review factors associated with the amplification of risk signals. We discuss these features of successful risk communication in relation to a range of specific examples, particularly opposition to community water fluoridation, Ebola, and routine childhood immunisation. (Hooker, et al., Public Health Res Pract. 2017)
https://www.ncbi.nlm.nih.gov/pubmed/28092105
Effectiveness of water fluoridation in the prevention of dental caries across adult age groups: CONCLUSION: Access to FW was associated with caries experience in Australian adults. The magnitude of associations varied between age groups, dependent on the natural history of caries and its measurement by DMFS. (Do, et al., Community Dent Oral Epidemiol. 2017)
https://www.ncbi.nlm.nih.gov/pubmed/27920310
Costs And Savings Associated With Community Water Fluoridation In The United States: Based on 2013 estimated costs ($324 million), net savings (savings minus costs) from fluoridation systems were estimated to be $6,469 million and the estimated return on investment, 20.0. While communities should assess their specific costs for continuing or implementing a fluoridation program, these updated findings indicate that program savings are likely to exceed costs. (O'Connell, Health Aff (Millwood). 2016)
https://www.ncbi.nlm.nih.gov/pubmed/28608827
Associations of Community Water Fluoridation with Caries Prevalence and Oral Health Inequality in Children:
These results suggest that CWF programmes are effective in the prevention of caries on permanent teeth and can reduce oral health inequalities among children. The implementation of CWF programmes should be sustained to overcome oral health inequalities due to socio-economic factors and improve children's overall oral health. (Kim, et al., Int J Environ Res Public Health. 2017)
https://www.ncbi.nlm.nih.gov/pubmed/27821097
The differences in healthcare utilization for dental caries based on the implementation of water fluoridation in South Korea:
RESULTS: Individuals with water fluoridation had a lower risk of dental care visits (HR = 0.949, 95 % CI = 0.928-0.971). Among the individuals who experienced a dental care visit, those with water fluoridation program had a lower number of dental care visits (β = -0.029), and the period of water fluoridation had an inverse association with the dental care expenditures.
CONCLUSION: The implementation of water fluoridation programs and these periods are associated with reducing the utilization of dental health care. Considering these positive impacts, healthcare professionals must consider preventive strategies for activating water fluoridation programs, such as changes in public perception and relations, for the effective management of dental care in South Korea. (Cho MS, et al. – BMC Oral Health. 2016 Nov 8;16(1):119)
https://www.ncbi.nlm.nih.gov/pubmed/27306248
Independent and Additive Effects of Different Sources of Fluoride and Dental Fluorosis:
CONCLUSION: In a community with water fluoridation, the factors associated with
dental fluorosis are intentional toothpaste ingestion and tooth-paste applied on
the whole toothbrush. (Celeste RK & Luz PB – Pediatr Dent. 2016;38(3):233-8)
https://www.ncbi.nlm.nih.gov/pubmed/27999493
ECONOMIC IMPORTANCE OF THE PREVENTIVE MEASURES IN DENTISTRY:
CONCLUSION: The importance of continuing education and local fluoridation is clearly reflected in the different values DMF-index, which was the subject of research. In the first group, in which is carried out continuous education and local fluoridation value of DMF index was 2.7, in the second group with local fluorination this value was 3.56, while in the third group, in which is not implemented preventive measures, the value DMF- index was 5.93. From an economic point the preventive measures are the cheapest, most effective and the best solution in order to maintain oral health.
(Deljo E, et al., & Mater Sociomed. 2016 Oct;28(5):397-401)
http://eprint.ncl.ac.uk/file_store/production/228428/30AD9B32-B931-4FF2-8E05-85DD56F83CFA.pdf
Fluoridation may not be linked with adverse health outcomes:
CONCLUSION: There was no
evidence for associations between fluoridation and nondental health outcomes such
as hip fracture, Down syndrome, osteosarcoma, all-cancer, or all-cause mortality. The authors concluded that their study provides reassurance that fluoridation
programs are a safe and highly effective way to provide a population with the
protective dental health property of fluoride. The study found lower rates of nondental outcomes in areas of artificial fluoridation. However, the authors stated
that the ecological study design did not allow any conclusions to be drawn with
regard to the potential protective effect of fluoridation for nondental outcomes.
(Blakey K & McNally RJ – J Evid Based Dent Pract. 2016 Sep;16(3):209-212)
https://www.ncbi.nlm.nih.gov/pubmed/26888380
Measuring the short-term impact of fluoridation cessation on dental caries in Grade 2 children using tooth surface indices:
CONCLUSIONS:
Trends observed for primary teeth were consistent with an adverse effect of fluoridation cessation on children's tooth decay, 2.5-3 years post-cessation. Trends for permanent teeth hinted at early indication of an adverse effect. It is important that future data collection efforts in the two cities be undertaken, to permit continued monitoring of these trends. (McLaren L,
et al. – Community Dent Oral Epidemiol. 2016 Jun;44(3):274-82)
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4484260
Water fluoridation and hypothyroidism:
Commentary on the 2015 Peckham et al hypothyroidism study.
The biggest problem with this paper, however, is in the interpretation which puts far too much weight on such weak evidence. The approach used is notoriously unreliable as a way of identifying independent associations and the lack of a clearly established prior hypothesis make it very unconvincing as evidence of a causal relationship. Given the other problems we have identified, this loose interpretation is a very serious concern. Such speculation is likely to result in unfounded public anxiety about a public health intervention which currently protects the health of children's teeth in many parts of the world. (John N Newton,
et al. – J Epidemiol Community Health. 2015 Jul; 69(7): 617–618)
https://www.ncbi.nlm.nih.gov/pubmed/27053119
Access to Fluoridated Water and Adult Dental Caries - A Natural Experiment:
Participants who accessed fluoridate water <50% of their lifetime presented a higher mean rate ratio of DMFT (1.39; 95% CI, 1.05-1.84) compared with those living >75% of their lifetime with residential access to fluoridated water. Participants living between 50% and 75% and <50% of their lives in fluoridated areas presented a decayed and filled teeth mean ratio of 1.34 (95% CI, 1.02-1.75) and 1.47 (95% CI, 1.05-2.04) higher than those with residential access to fluoridated water >75% of their lifetime, respectively. Longer residential lifetime access to fluoridated water was associated with less dental caries even in a context of multiple exposures to fluoride. (Peres MA,
et al. – J Dent Res. 2016 Jul;95(8):868-74)
https://www.ncbi.nlm.nih.gov/pubmed/27177581
Does cessation of community water fluoridation lead to an increase in tooth decay? A systematic review of published studies:
CONCLUSIONS: Overall, the published research points more to an increase in dental caries post-CWF cessation than otherwise. However, the literature is highly diverse and variable in methodological quality. (McLaren L & Singhal S
– J Epidemiol Community Health. 2016 Sep;70(9):934-40)
https://www.ncbi.nlm.nih.gov/pubmed/27467460
Comparative effectiveness of water and salt community-based fluoridation methods in preventing dental caries among schoolchildren:
CONCLUSION: Fluoridated water appears to provide a better protective effect against dental caries than fluoridated household salt among schoolchildren from developing countries. (Fabruccini A,
et al. – Community Dent Oral Epidemiol. 2016 Jul 28)
https://www.ncbi.nlm.nih.gov/pubmed/27678306
Dental caries, fluorosis, oral health determinants, and quality of life in adolescents: CONCLUSION: Increased impact on oral health-related quality of life (OHRQoL) was related to the severity of cavitated dentine lesions, but fluorosis resulting from combined fluoride exposure from early ages was not of concern for the adolescents.
CLINICAL RELEVANCE: Combined fluoride exposure from fluoridated drinking water, consumption of food prepared with fluoridated water, and daily twice brushing with conventional fluoride toothpaste from early ages may be recommended to control caries progression at population level without impact on OHRQoL. This information is particularly relevant for supporting oral health police for disadvantaged populations. (Aimée NR,
et al. – Clin Oral Investig. 2016 Sep 27)
https://www.ncbi.nlm.nih.gov/pubmed/26762869
Evaluation of optimal water fluoridation on the incidence and skeletal distribution of naturally arising osteosarcoma in pet dogs:
Taken together, these analyses do not support the hypothesis that optimal fluoridation of drinking water contributes to naturally occurring osteosarcoma in dogs. (Rebhun RB,
et al. – Vet Comp Oncol. 2016 Jan 14)
https://www.ncbi.nlm.nih.gov/pubmed/26776927
Economic Evaluation of Community Water Fluoridation: A Community Guide Systematic Review:
EVIDENCE SYNTHESIS: The analysis was conducted in 2014. The benefit-only studies used regression analysis, showing that different measures of dental costs were always lower in communities with water fluoridation. For the six cost-benefit studies, per capita annual intervention cost ranged from $0.11 to $4.92 for communities with at least 1,000 population, and per capita annual benefit ranged from $5.49 to $93.19. Benefit-cost ratios ranged from 1.12:1 to 135:1, and these ratios were positively associated with community population size.
CONCLUSIONS: Recent evidence continues to indicate that the economic benefit of community water fluoridation exceeds the intervention cost. Further, the benefit-cost ratio increases with the community population size. (Ran T,
et al. – Am J Prev Med. 2016 Jun;50(6):790-6)
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5010502
Cost-effectiveness of preventing dental caries and full mouth dental reconstructions among Alaska Native children in the Yukon–Kuskokwim delta region of Alaska:
Water Fluoridation: Adjusting the level of fluoride in the community water systems results in a 26-35 percent reduction in tooth decay among children receiving lifelong exposure to fluoridated water. Other estimates based earlier YK dental reviews suggests 18-40 percent reduction in tooth decay among children receiving community fluoridated water. (Charisma Y. Atkins,
et al. – J Public Health Dent. 2016 Jun; 76(3): 228–240)
https://www.ncbi.nlm.nih.gov/pubmed/26680434
Public perceptions and scientific evidence for perceived harms/risks of community water fluoridation: An examination of online comments pertaining to fluoridation cessation in Calgary in 2011:
OBJECTIVES: To examine the perceived harms/risks of fluoridation as expressed in online forums relating to cessation and aftermath in Calgary, specifically, 1) which harms/risks are mentioned, 2) for those harms/risks, what kinds of evidence are cited, 3) to what extent is scientific literature cited, and what is its quality, and 4) for a subset of harms/risks, what is known from the broader scientific literature?
METHODS: Relevant online comments were identified through free-text Internet searches, and those explicitly discussing the harms/risks of water fluoridation were extracted. Types of evidence mentioned were identified, and the scientific papers cited were reviewed. Finally, the broader scientific literature on two of the harms/risks was reviewed and synthesized.
SYNTHESIS: We identified 17 distinct groups of harms/risks, which spanned human body systems, the environment and non-human organisms. Most often, no evidence was cited. When evidence was cited, types included individuals viewed as authorities and personal experiences. Reference to scientific articles was rare, and those papers (n = 9) had significant methodological concerns. Our review of scientific literature on fluoride and 1) thyroid functioning and 2) phytoplankton revealed some negative effects of fluoride at concentrations exceeding maximum recommended levels (>1.5 ppm).
CONCLUSION: The findings have implications for communication with the public about fluoridation. First, to the extent that the public consults the scientific literature, it is essential that the methodological limitations of a study, as well as its relevance to community water fluoridation, be widely and promptly communicated. Second, scientific evidence is only one component of why some people support or do not support fluoridation, and communication strategies must accommodate that reality. (Podgorny PC & McLaren L.
– Can J Public Health. 2015 Jun 19;106(6):e413-25)
https://www.ncbi.nlm.nih.gov/pubmed/26738215
Long-term evaluation of the clinical effectiveness of community milk fluoridation in Bulgaria:
CONCLUSIONS: Fluoridated milk delivered daily in schools in Bulgaria resulted in substantially lower caries development compared with children in schools receiving milk without added fluoride. The nation-wide experiences from milk fluoridation indicate that such a public health scheme can be effective to the global fight against dental caries of children. (Petersen PE,
et al. – Community Dent Health. 2015 Dec;32(4):199-203)
https://www.ncbi.nlm.nih.gov/pubmed/26715525
Association between estimated fluoride intake and dental caries prevalence among 5-year-old children in Korea:
CONCLUSION: The inverse association between dietary fluoride intake levels and prevalence of dental caries implies that the introduction of community caries prevention programmes may be beneficial. Such programmes would include water fluoridation and a fluoride supplementation programme. (Kim MJ,
et al. – BMC Oral Health. 2015 Dec 30;15:169)
https://www.ncbi.nlm.nih.gov/pubmed/25899748
Factors attributable for the prevalence of dental caries in Queensland children:
In the full models, children in the nonfluoridated areas had significantly higher prevalence of dental caries [PR for the primary: 1.29 (1.11-1.50); PR for the permanent 1.49 (1.01-2.21)] compared with children in fluoridated areas, controlling for other factors. PAF estimates indicated that lack of water fluoridation attributed to 21% and 31% of primary and permanent dental caries, respectively in this child population. (Do LG.,
et al. – Community Dent Oral Epidemiol. 2015 Oct;43(5):397-405)
https://www.ncbi.nlm.nih.gov/pubmed/26092033
(full
review)
Water fluoridation for the prevention of dental caries
- Cochrane Review:
The results from the caries severity data
indicate that the initiation of water fluoridation results in reductions
in dmft of 1.81 (95% CI 1.31 to 2.31; 9 studies at high risk of bias, 44,268
participants) and in DMFT of 1.16 (95% CI 0.72 to 1.61; 10 studies at high
risk of bias, 78,764 participants). This translates to a 35% reduction in
dmft and a 26% reduction in DMFT compared to the median control group mean
values. There were also increases in the percentage of caries free children
of 15% (95% CI 11% to 19%; 10 studies, 39,966 participants) in deciduous
dentition and 14% (95% CI 5% to 23%; 8 studies, 53,538 participants) in
permanent dentition. The majority of studies (71%) were conducted prior
to 1975 and the widespread introduction of the use of fluoride toothpaste.There
is insufficient information to determine whether initiation of a water fluoridation
programme results in a change in disparities in caries across socioeconomic
status (SES) levels.There is insufficient information to determine the effect
of stopping water fluoridation programmes on caries levels.No studies that
aimed to determine the effectiveness of water fluoridation for preventing
caries in adults met the review's inclusion criteria.With regard to dental
fluorosis, we estimated that for a fluoride level of 0.7 ppm the percentage
of participants with fluorosis of aesthetic concern was approximately 12%
(95% CI 8% to 17%; 40 studies, 59,630 participants). This increases to 40%
(95% CI 35% to 44%) when considering fluorosis of any level (detected under
highly controlled, clinical conditions; 90 studies, 180,530 participants).
Over 97% of the studies were at high risk of bias and there was substantial
between-study variation. (Cochrane Database Syst Rev. 2015 Jun 18;6)
(a
response to feedback)
There was significant resulting
commentary (#1,
#2,
#3,
#4,
#5,
#6,
#7) that clearly illustrates the complexity of the fluoridation discussion,
the way a published paper can be misused by fluoridation opponents and the
impact of personal biases (for and against fluoridation) on the interpretation
of study results. Contrast the 2015 Cochrane review with a 2000 literature
review of fluoridation,
Systematic review of water fluoridation, published in the British
Medical Journal that concluded, "The
evidence of a beneficial reduction in caries should be considered together
with the increased prevalence of dental fluorosis. There was no clear evidence
of other potential adverse effects."
https://www.ncbi.nlm.nih.gov/pubmed/26153549
Community water fluoridation and health outcomes in England: a cross-sectional study:
BACKGROUND: Six million people in England live in areas where the level of fluoride in water is adjusted to reduce the significant public health burden of dental caries. The dental effects of fluoride are well established, but evidence for suggested adverse health effects is limited, with a lack of rigorous small area population studies that control for confounding. This study aims to test the association between water fluoridation schemes and selected health outcomes using the best available routine data sources.
METHODS: Ecological level exposure to fluoridated water was estimated for standard small areas and administrative districts in England using Geographical Information Systems and digitized boundaries based on known patterns of water supply. The association between fluoridation and dental and nondental health indicators was tested using multivariable regression models including ecological level confounding variables. Health indicator data were obtained from routine sources.
RESULTS: There was strong evidence of lower prevalence of dental caries (P< 0.001) among children living in fluoridated areas, they also had fewer teeth affected on average (P
< 0.001), and lower admission rates for tooth extraction (55% lower; 95% CI-73%, -27%; P = 0.001). There was no strong evidence of an association between fluoridation and hip fracture, Down syndrome, all-cancer, all-cause mortality or osteosarcoma. Fluoridation was negatively associated with the incidence of renal stones (7.9% lower; 95% CI-9.6%,-6.2%; P
< 0.001) and bladder cancer (8.0% lower; 95% CI-9.9%,-6.0%; P < 0.001).
CONCLUSION: This study uses the comprehensive data sets available in England to provide reassurance that fluoridation is a safe and highly effective public health measure to reduce dental decay. Although lower rates of certain nondental outcomes were found in fluoridated areas, the ecological, observational design prohibits any conclusions being drawn regarding a protective role of fluoridation.
(Young N, et al. – Community Dent Oral Epidemiol. 2015 Dec;43(6):550-9)
Community Water Fluoridation in New Zealand
A cost effectiveness analysis of community water fluoridation in New Zealand:
This cost effectiveness analysis supports an earlier economic analysis of community water fluoridation in New Zealand by Wright et. al. (2001) 3 . CWF remained a cost effective public health intervention in New Zealand despite an overall reduction in dental caries. This finding also agrees with a number of economic analyses of CWF conducted in countries similar to New Zealand, 7, 9-11 . It should be noted however, that for smaller communities cost effectiveness was more marginal. Wright et. al. (2001) identified a ‘break even’ community size for CWF of 700-900 people 3 . In smaller communities cost effectiveness was more dependent on the risk profile of the population. CWF would be more cost effective in communities with a higher risk of dental caries.
(Fyfe C, et al. – New Zealand Medical Journal 12/2015, 128(1427))
https://www.ncbi.nlm.nih.gov/pubmed/26680434
Public perceptions and scientific evidence for perceived harms/risks of community water fluoridation: An examination of online comments pertaining to fluoridation cessation in Calgary in 2011:
OBJECTIVES: To examine the perceived harms/risks of fluoridation as expressed in online forums relating to cessation and aftermath in Calgary, specifically, 1) which harms/risks are mentioned, for those harms/risks, what kinds of evidence are cited, to what extent is scientific literature cited, and what is its quality, and for a subset of harms/risks, what is known from the broader scientific literature?
METHODS: Relevant online comments were identified through free-text Internet searches, and those explicitly discussing the harms/risks of water fluoridation were extracted. Types of evidence mentioned were identified, and the scientific papers cited were reviewed. Finally, the broader scientific literature on two of the harms/risks was reviewed and synthesized.
SYNTHESIS: We identified 17 distinct groups of harms/risks, which spanned human body systems, the environment and non-human organisms. Most often, no evidence was cited. When evidence was cited, types included individuals viewed as authorities and personal experiences. Reference to scientific articles was rare, and those papers (n = 9) had significant methodological concerns. Our review of scientific literature on fluoride and thyroid functioning and phytoplankton revealed some negative effects of fluoride at concentrations exceeding maximum recommended levels (>1.5 ppm).
CONCLUSION:
The findings have implications for communication with the public about fluoridation. First, to the extent that the public consults the scientific literature, it is essential that the methodological limitations of a study, as well as its relevance to community water fluoridation, be widely and promptly communicated. Second, scientific evidence is only one component of why some people support or do not support fluoridation, and communication strategies must accommodate that reality.
(Podgorny PC, McLaren L. – Can J Public Health. 2015 Jun 19;106(6))
http://www.jcda.ca/water-fluoridation-safety-effectiveness-and-value-oral-health-symposium-2014-annual-meeting-american
Water Fluoridation: Safety, Effectiveness and Value in Oral Health: A Symposium at the 2014 Annual Meeting of the American and Canadian Associations for Dental Research:
The objective of this symposium was to review the scientific evidence supporting CWF and consider the implications for optimizing the use of fluoride in public health and clinical practice. The following presentations were held at the symposium:
1. Effectiveness of fluorides - Findings of evidence-based reviews:
The use of fluoride has been associated with a substantial reduction in caries in children and adolescents. The presentation also highlighted evidence gaps for effectiveness of certain fluoride modalities, as well as the relationship among effectiveness, dose, and safety for the products. With the exception of enamel fluorosis, no other adverse effects are associated with community water fluoridation.
2. The health assessment of fluoride in drinking water: Conclusions from the National Research Council and subsequent scientific assessments by EPA:
a) EPA estimates of RfD and the recommended benchmarks are conservative.
b) More recent studies of osteosarcoma and bone fractures confirm that water fluoridation has no impact on these outcomes.
c) Lowering fluoride exposure may lead to reduction in dental fluorosis but the question remains about its impact on caries.
3. Gaps in scientific knowledge regarding water fluoridation and other fluoride modalities: Fluoridated water reduces tooth decay in adults, even if they start drinking it after childhood. Communities that implement fluoridation can expect benefits to accrue for both future and current generations. More people in the population benefit from water fluoridation than previously was thought. The greater benefit has a significant impact on calculations of population cost-effectiveness. Recent findings from Australia add to six decades of evidence showing that community water fluoridation prevents dental caries in adults. The evidence should be considered when formulating health policies and public health programs.
4. Community water fluoridation: Translating evidence into public health practice: The translation of scientific evidence into public health practice demands ongoing efforts to update estimates of effectiveness and costs of the intervention, assure safety, identify and address gaps in knowledge, and apply data-driven approaches to monitor implementation and communicate with stakeholders.
(Presenters, Dr. Martinez-Mier, Dr. Kumar, Dr. Slade, Dr. Gooch – J Can Dent Assoc 2015;81:f16)
https://www.ncbi.nlm.nih.gov/pubmed/25327814
Does fluoride in the water close the dental caries gap between Indigenous and non-Indigenous children?
RESULTS: Dental caries prevalence and severity for Indigenous and non-Indigenous children, in both dentitions, was lower in fluoridated areas compared to non-fluoridated areas. Among non-Indigenous children, there was a 50.9% difference in mean dmft scores in fluoridated (1.70) compared to non-fluoridated (2.86) areas. The difference between Indigenous children in fluoridated (3.29) compared to non-fluoridated (4.16) areas was 23.4%. Among non-Indigenous children there was a 79.7% difference in the mean DMFT scores in fluoridated (0.68) compared to non-fluoridated (1.58) areas. The difference between Indigenous children in fluoridated (1.59) and non-fluoridated (2.23) areas was 33.5%.
CONCLUSIONS: Water fluoridation is effective in reducing dental caries, but does not appear to close the gap between non-Indigenous children and Indigenous children.
(Lalloo R, et al. – Aust Dent J. 2015 Sep;60(3):390-6)
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4547570
U.S. Public Health Service Recommendation for Fluoride Concentration in Drinking Water for the Prevention of Dental Caries:
Through this final recommendation, the U.S. Public Health Service (PHS) updates and replaces its 1962 Drinking Water Standards related to community water fluoridation—the controlled addition of a fluoride compound to a community water supply to achieve a concentration optimal for dental caries prevention.1 For these community water systems that add fluoride, PHS now recommends an optimal fluoride concentration of 0.7 milligrams/liter (mg/L). In this guidance, the optimal concentration of fluoride in drinking water is the concentration that provides the best balance of protection from dental caries while limiting the risk of dental fluorosis. The earlier PHS recommendation for fluoride concentrations was based on outdoor air temperature of geographic areas and ranged from 0.7–1.2 mg/L.
Systematic reviews of the scientific evidence related to fluoride have concluded that community water fluoridation is effective in decreasing dental caries prevalence and severity. Effects included significant increases in the proportion of children who were caries-free and significant reductions in the number of teeth or tooth surfaces with caries in both children and adults. When analyses were limited to studies conducted after the introduction of other sources of fluoride, especially fluoride toothpaste, beneficial effects across the lifespan from community water fluoridation were still apparent.
Fluoride in saliva and dental plaque works to prevent dental caries primarily through topical -remineralization of tooth surfaces. Consuming fluoridated water and beverages, and foods prepared or processed with fluoridated water, throughout the day maintains a low concentration of fluoride in saliva and plaque that enhances remineralization. Although other fluoride-containing products are available and contribute to the prevention and control of dental caries, community water fluoridation has been identified as the most cost-effective method of delivering fluoride to all members of the community regardless of age, educational attainment, or income level.9,30 Studies continue to find that community water fluoridation is cost saving. (Public Health Rep. 2015 Jul-Aug; 130(4): 318–331)
https://www.ncbi.nlm.nih.gov/pubmed/26346578
Water Intake by Outdoor Temperature Among Children Aged 1-10 Years: Implications for Community Water Fluoridation in the U.S.
RESULTS: We found that total water intake was not associated with temperature. Plain water intake was weakly associated with temperature in unadjusted (coefficient 5 0.2, p=0.015) and adjusted (coefficient 5 0.2, p=0.013) linear regression models. However, these models explained little of the individual variation in plain water intake (unadjusted: R(2)=0.005; adjusted: R(2)=0.023).
CONCLUSION: Optimal fluoride concentration in drinking water to prevent caries need not be based on outdoor temperature, given the lack of association between total water intake and outdoor temperature, the weak association between plain water intake and outdoor temperature, and the minimal amount of individual variance in plain water intake explained by outdoor temperature. These findings support the change in the U.S. Public Health Service recommendation for fluoride concentration in drinking water for the prevention of dental caries from temperature-related concentrations to a single concentration that is not related to outdoor temperature.
(Beltrán-Aguilar ED, et al. – Public Health Rep. 2015 Jul-Aug;130(4):362-71)
https://www.ncbi.nlm.nih.gov/pubmed/26285190
Risk perception, psychological heuristics and the water fluoridation controversy:
OBJECTIVES: Increasingly, support for water fluoridation has come under attack. We seek an explanation, focusing on the case of Waterloo, Ontario, where a 2010 referendum overturned its water fluoridation program. In particular, we test whether individuals perceive the risks of water fluoridation based not on 'hard' scientific evidence but on heuristics and cultural norms.
METHODS: A sample of 376 residents in Waterloo were surveyed in June 2012 using random digit dialing. We use factor analysis, OLS regression, as well as t-tests to evaluate a survey experiment to test the credibility hypothesis.
RESULTS: Perceptions of fluoride as a risk are lower among those who perceive fluoride's benefits (B = .473, p < 0.001) and those whose cultural view is 'egalitarian' (B = .156, p < 0.05). The experiment shows a lower level of perception of fluoride's benefits among respondents who are told that water fluoridation is opposed by a national advocacy group (Group A) compared to those who are told that the government and the World Health Organization support fluoridation (Group B) (t = 1.6547, p < 0.05), as well as compared to the control group (t = 1.8913, p < 0.05). There is no difference between Group B and the control, possibly because people's already general support for fluoridation is less prone to change when told that other public organizations also support fluoridation.
CONCLUSION: Public health officials should take into account cultural norms and perceptions when individuals in a community appear to rise up against water fluoridation, with implications for other public health controversies.
(Perrella AM, Kiss SJ – Can J Public Health. 2015 Apr 29;106-10)
http://www.publish.csiro.au/?act=view_file&file_id=HEv26n1_ED.pdf
New international review supports community water fluoridation as an effective and safe dental health promotion measure:
Strong evidence supports the safety and efficacy of CWF. The benefits are most pronounced for low SES groups. However, opponents of fluoridation through dissemination of misinformation pose an ongoing threat to CWF’s continuation. Public health professionals have a responsibility to counter such misinformation and to support water fluoridation.
(Howat P, et al. – Health Promotion Journal of Australia, 2015, 26, 1–3)
https://www.ncbi.nlm.nih.gov/pubmed/25913418
A 4-year assessment of a new water-fluoridation scheme in New South Wales, Australia:
OBJECTIVE: To monitor the changes in dental caries prevalence of 5- to 7-year-old children living in a fluoridated area, a newly fluoridated area and in an area without water fluoridation, in NSW, Australia.
RESULTS: The caries prevalence changed over time. In 2008, the mean dmft index was 1.40 for the fluoridated area, 2.02 for the area about to fluoridate and 2.09 for the unfluoridated control. By 2012, these mean dmft scores were 0.69, 0.72 and 1.21, respectively. In the two areas where children received fluoridated water, the significant caries index was 2.30 for the fluoridated area and 2.40 for the newly fluoridated area. The significant caries score for children in the unfluoridated location was 3.93. Multivariate analysis showed that over time the differences in dental caries prevalence between the established fluoride area and the newly fluoridated area diminished. However, children in the unfluoridated control area continued to demonstrate significant differences in the mean number of decayed teeth compared with children in the fluoridated comparator sites, and the proportions of children free from decay were significantly higher in the fluoridated areas than in the unfluoridated area.
CONCLUSION: Fluoridation of public water supplies in Gosford and Wyong offers young children better dental health than those children who do not have access to this public health measure.
(Blinkhorn AS, et al. – Int Dent J. 2015 Jun;65(3):156-63)
https://www.ncbi.nlm.nih.gov/pubmed/25816847
Does lower lifetime fluoridation exposure explain why people outside capital cities have poor clinical oral health?
BACKGROUND: Australians outside state capital cities have greater caries experience than their counterparts in capital cities. We hypothesized that differing water fluoridation exposures was associated with this disparity.
METHODS: Data were the 2004-06 Australian National Survey of Adult Oral Health. Examiners measured participant decayed, missing and filled teeth and DMFT Index and lifetime fluoridation exposure was quantified. Multivariable linear regression models estimated differences in caries experience between capital city residents and others, with and without adjustment for fluoridation exposure.
RESULTS: There was greater mean lifetime fluoridation exposure in state capital cities (59.1%, 95% confidence interval=56.9,61.4) than outside capital cities (42.3, confidence interval=36.9,47.6). People located outside capital city areas had differing socio-demographic characteristics and dental visiting patterns, and a higher mean DMFT (Capital cities=12.9, Non-capital cities=14.3, p=0.02), than people from capital cities. After adjustment for socio-demographic characteristics and dental visits, DMFT of people living in capital cities was less than non-capital city residents (Regression coefficient=0.8, p=0.01). The disparity was no longer statistically significant (Regression coefficient=0.6, p=0.09) after additional adjustment for fluoridation exposure.
(Crocombe LA, et al. – Aust Dent J. 2015 Mar 26)
http:447426/
Fluoridation and hypothyroidism – a commentary on Peckham et al. -
Peckham et al. fail to understand the limitations of a poorly conducted ecological trial, and the paper contains serious biases and flaws. Literature reviews have been highly selective and critical analysis of that literature has been poor. The authors show a disturbing tendency to focus on a small number of poor quality studies that reinforce their own views, while ignoring contradictory evidence from much stronger studies and reviews. Peckham et al. should have heeded the adage ‘correlation is not causation’ before coming to a conclusion at odds with a large body of reputable evidence from around the world. In my opinion, the paper’s conclusions can and should be dismissed.
(M. Foley – British Dental Journal, Vol. 219,9, 11/13/2015)
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4447426/
Exposure to fluoride in drinking water and hip fracture risk: a meta-analysis of observational studies:
CONCLUSION: The present meta-analysis suggests that chronic fluoride exposure from drinking water does not significantly increase the risk of hip fracture. Given the potential confounding factors and exposure misclassification, further large-scale, high-quality studies are needed to evaluate the association between exposure to fluoride in drinking water and hip fracture risk.
(Yin XH, et al. – PLoS One. 2015 May 28)
https://www.ncbi.nlm.nih.gov/pubmed/25327339
Water fluoridation, dentition status and bone health of older people
in Ireland:
RESULTS: It was found that the greater the percentage
of households with a fluoridated water supply in an area, the higher the
probability that respondents had all their own teeth. There was no significant
relationship between the proportion of households with a fluoridated water
supply in an area and bone health.
CONCLUSION: This study suggests that
water fluoridation provides a net health gain for older Irish adults, though
the effects of fluoridation warrant further investigation. (O Sullivan V,
O Connell BC. – Community Dent Oral Epidemiol. 2015 Feb;43(1):58-67)
A description of the study can be
read here/a>.
https://www.ncbi.nlm.nih.gov/pubmed/25661315
Effects of water fluoridation on caries experience in the primary dentition
in a high caries risk community in Queensland, Australia: CONCLUSIONS:
After only 36 months of water fluoridation there was a significant drop
in caries prevalence from 87 to 75% and a 19% reduction in caries experience
in a community with one of the highest caries rates in Australia.
(Koh R, et al. – Caries Res. 2015;49(2):184-91)
https://www.ncbi.nlm.nih.gov/pubmed/26147330
Perceived safety and benefit of community water fluoridation: 2009 HealthStyles survey:
CONCLUSIONS: Although only a minority of the US population perceived CWF as unsafe or providing no benefit to health, perceptions regarding CWF varied by knowledge of CWF and socio-demographic factors. Oral health promotion activities should consider these differing perceptions of CWF among groups to tailor oral health messaging appropriately.
(Mork N, Griffin S. – J Public Health Dent. 2015 Sep;75(4):327-36)
https://www.ncbi.nlm.nih.gov/pubmed/25726345
Hospitalizations for dental infections: Optimally versus nonoptimally
fluoridated areas in Israel: CONCLUSIONS: These results clearly
indicate that there is an association between adequacy of water fluoridation
and hospitalization due to dental infections among children and adolescents.
This effect is more prominent in populations of lower socioeconomic status.
(Klivitsky A, et al. – J Am Dent Assoc. 2015 Mar; 146(3):179-83)
https://www.ncbi.nlm.nih.gov/pubmed/24832151
Full Article
Community Water Fluoridation and Intelligence: Prospective
Study in New Zealand:
Objectives. This study aimed
to clarify the relationship between Community Water Fluoridation (CWF) and
IQ.
Methods. We conducted a prospective study of a general population
sample of those born in Dunedin, New Zealand, between April 1, 1972, and
March 30, 1973 (95.4% retention of cohort after 38 years of prospective
follow-up). Residence in a CWF area, use of fluoride dentifrice and intake
of 0.5-milligram fluoride tablets were assessed in early life (prior to
age 5 years); we assessed IQ repeatedly between ages 7 to 13 years and at
age 38 years.
Results. No clear differences in IQ because of
fluoride exposure were noted. These findings held after adjusting for potential
confounding variables, including sex, socioeconomic status, breastfeeding,
and birth weight (as well as educational attainment for adult IQ outcomes).
Conclusions. These findings do not support the assertion
that fluoride in the context of CWF programs is neurotoxic. Associations
between very high fluoride exposure and low IQ reported in previous studies
may have been affected by confounding, particularly by urban or rural status.
(Broadbent JM, et al. – Am J Public Health. 2015 Jan;105(1):72-76)
https://www.ncbi.nlm.nih.gov/pubmed/256046255
The Dental Health of primary school children living in fluoridated, pre-fluoridated
and non-fluoridated communities in New South Wales, Australia:
CONCLUSION: The children living in the well-established fluoridated area
had less dental caries and a higher proportion free from disease when compared
with the other two areas which were not fluoridated. Fluoridation demonstrated
a clear benefit in terms of better oral health for young children. (Blinkhorn
AS, et al. – BMC Oral Health. 2015 Jan 21;15(1):9)
Setting the Record Straight on Fluoride: In a letter to JAMA Internal Medicine published earlier this year, two political scientists from the University of Chicago reported that 12% of Americans agree with this statement: “Public water fluoridation is really just a secret way for chemical companies to dump the dangerous byproducts of phosphate mines into the environment.” Perhaps more disturbing, fewer than half of respondents disagreed with the statement, which means there is an urgent need to steer people toward reliable sources of accurate information so they can play an informed role in decision-making around this crucial aspect of the public health infrastructure.
(Valachovic R. – J Mich Dent Assoc. 2015 Apr;97(4):38-40)
https://www.ncbi.nlm.nih.gov/pubmed/255588977
Contemporary multilevel analysis of the effectiveness of water fluoridation
in Australia: RESULTS: Data from 2,214 5-8 year-olds and 3,186
9-14 year-olds from 207 schools in 16 areas were analysed. Queensland's
average dmfs was 4.23 and DMFS 1.47. The lowest levels of dental caries
were observed in long-term fluoridated Townsville. In the full models, Townsville
children had significantly lower caries experience (RR for dmfs: 0.61
(95%CI: 0.44-0.82); RR for DMFS 0.60 (95%CI: 0.42-0.88)) compared with
children in non-fluoridated areas. (Do L, Spencer AJ. – Aust N Z J Public Health.
2015 Feb;39(1):44-50)
https://www.ncbi.nlm.nih.gov/pubmed/255110822
Dental fluorosis in the Blue Mountains and Hawkesbury, New South Wales,
Australia: policy implications: CONCLUSIONS: For the group as
a whole, we concluded that: (a) fluorosis prevalence (0.39) in both regions
was similar; and (b) the higher-than-expected prevalence and severity of
fluorosis was due mainly to two factors: (a) the higher-than-optimal fluoride
level in drinking water; and (b) swallowing of fluoride toothpaste in early
childhood. (Bal IS, et al. – J Investig Clin Dent. 2015 Feb;6(1):45-52)
A related letter to the BDJ
From the American Academy of Pediatrics
Fluoride Use in Caries Prevention in the Primary Care Setting: Dental caries remains the most common chronic disease of childhood in the United States. Caries is a largely preventable condition, and fluoride has proven effectiveness in the prevention of caries. The goals of this clinical report are to clarify the use of available fluoride modalities for caries prevention in the primary care setting and to assist pediatricians in using fluoride to achieve maximum protection against dental caries while minimizing the likelihood of enamel fluorosis.
(Clark M, et al. – Pediatrics Vol. 134 No. 3 September 1, 2014 pp. 626 -633)
North Carolina Medical Journall
Preventing Dental Caries Through
Community Water Fluoridation: The weight of the scientific evidence
in peer-reviewed literature does not support an association between community
water fluoridation and any adverse health effects or systemic disorders,
including an increased risk for cancer, Down syndrome, heart disease, osteoporosis,
bone fractures, immune disorders, low intelligence, renal disorders, Alzheimer
disease, or allergic reactions. Not only is community water fluoridation
safe and effective, it is also cost saving, and it is the least expensive
way to deliver the benefits of fluoride to all residents of a community.
(White BA & Gordon SM – N C Med J. 2014;75(6):430-431) {A summary of
benefits from a review of other papers}
https://www.ncbi.nlm.nih.gov/pubmed/25364597
- Free
Full Text
Dental Fluorosis and Dental Caries Prevalence among
12 and 15-Year-Old School Children in Nalgonda District, Andhra Pradesh,
India:
BACKGROUND: Fluoride is a double edged sword. The
assessment of dental caries and fluorosis in endemic fluoride areas will
facilitate in assessing the relation between fluoride concentrations in
water with dental caries, dental fluorosis simultaneously.
RESULTS:
The caries prevalence was less among 12-year-old children (39.9%]) compared
with 15-years-old children (46.7%). The prevalence was more among females
(50.4% than males (35.8%. The prevalence was more in low fluoride area (60.5%)
followed by very high fluoride area (54.8%), high fluoride area (32.4%])
and medium fluoride area (17.6%) in the descending order. The fluorosis
prevalence increased with increasing fluoride concentration with no difference
in gender and age distribution.
CONCLUSION: Low fluoride areas require
fluoridation or alternate sources of fluoride, whereas high fluoride areas
require defluoridation. Defluoridation of water is an immediate requirement
in areas with fluoride concentration of 4 parts per million and above as
dental fluorosis is a public health problem in these areas with 100% prevalence.
(Sukhabogi Jr, et al. – Ann Med Health Sci Res. 2014 Sep;4(Suppl 3))
https://www.ncbi.nlm.nih.gov/pubmed/2532942666
The effect of lifetime fluoridation exposure on dental caries experience
of younger rural adults: CONCLUSIONS: The higher level of lifetime
fluoridation exposure was associated with substantially lower caries experience
in younger rural adults, largely due to a lower number of filled teeth.
(Crocombe L, et al. – Aust Dent J. 2014 Oct 20.)
https://www.ncbi.nlm.nih.gov/pubmed/25448884
Variation in fluorosis and caries experience among Lithuanian 12 year olds exposed to more than 1 ppm F in tap water:
AIM: The aim of the present study was to analyze caries experience in relation to the occurrence of fluorosis in 12 year olds in a natural fluoride area.
CONCLUSION: The presence of fluorosis associates with lesser caries experience in 12-year-old lifetime residents of an area with moderately-elevated natural fluoride.
(Narbutaitė J, et al. – J Investig Clin Dent. 2014 Dec 1)
https://www.ncbi.nlm.nih.gov/pubmed/2516676161
Fluoride retention in saliva and in dental biofilm after different home-use
fluoride treatments: In this study, we evaluated whether fluoride
concentrations in saliva and dental biofilm remained significantly elevated
at 8 h after four different oral hygiene procedures in volunteers living
in an area with fluoridated water supply. The fluoride concentrations in
saliva and in dental biofilm were not significantly different among the
treatments. The frequency of brushing with a fluoride dentifrice and additional
use of fluoride mouthrinse followed by brushing with a fluoride dentifrice
did not affect the fluoride concentrations in biofilm and saliva at 8 h
after the last procedure. The results of this study are in agreement with
the findings of most of the studies conducted in areas with a fluoridated
water supply.13,20,21,22 These studies also did not show a long-term effect
on the fluoride concentration in saliva and in dental biofilm compared to
baseline values. A possible explanation for these is that plaque-binding
sites for long-term fluoride retention are occupied by fluoride ions largely
in communities with fluoridated water, but not where the water contains
only traces of this ion. (Souza DC & Maltz M. – Braz Oral Res. 2014 Jan-Feb;28)
British Dental Journal
Concern over limited access to water
fluoridation: The British Dental Association (BDA) and the British
Society of Paediatric Dentistry (BSPD) have expressed concern that limited
access to water fluoridation - only 10% of the UK's population - means we
are failing children who live in communities with high levels of tooth decay.
Concern over limited access to water fluoridation In its latest report on
fluoridation, the BSPD highlights that 60,683 children and adolescents in
England were admitted to hospital in 2012/13 to have multiple decayed teeth
removed under general anaesthetic, costing the NHS at least '27.6 million.
By contrast, evidence suggests that children living in fluoridated areas,
such as the West Midlands, have around half the rate of tooth decay of those
living in non-fluoridated areas, and thousands have been spared from traumatic
and distressing operations. Research indicates that adults also benefit.
(British Dental Journal 217, 616 (2014))
https://www.ncbi.nlm.nih.gov/pubmed/2460327070
An alternative marker for the effectiveness of water fluoridation: hospital
extraction rates for dental decay, a two-region study: CONCLUSIONS:
After ranking by IMD, DSRs of hospital admissions for the extraction of
decayed or pulpally/periapically involved teeth is lower in areas with a
fluoridated water supply. The analysis of routinely collected HES data may
help identify the impact of water fluoridation schemes. (Elmer TB, et
al. – Br Dent J. 2014 Mar;216(5))
https://www.ncbi.nlm.nih.gov/pubmed/25230407
Community water fluoridation on the Internet and social media:
OBJECTIVES:
In the United States, 95 percent of teens and 85 percent of adults use the
Internet. Two social media outlets, Facebook and Twitter, reach more than
150 billion users. This study describes anti-fluoridation activity and dominance
on the Internet and social media, both of which are community water fluoridation
(CWF) information sources.
METHODS: Monthly website traffic to
major fluoridation websites was determined from June 2011 to May 2012. Facebook,
Twitter, and YouTube fluoridation activity was categorized as "proCWF" or
"anti-CWF." Twitter's anti-CWF tweets were further subcategorized by the
argument used against CWF.
RESULTS: Anti-CWF website traffic
was found to exceed proCWF activity five- to sixty-fold. Searching "fluoride"
and "fluoridation" on Facebook resulted in 88 to 100 percent anti-CWF groups
and pages; "fluoridation" on Twitter and YouTube resulted in 64 percent
anti-CWF tweets and 99 percent anti-CWF videos, respectively. "Cancer, "
"useless, " and "poisonous" were the three major arguments used against
fluoridation.
CONCLUSIONS: Anti-fluoridation information significantly
dominates the Internet and social media. Thousands of people are being misinformed
daily about the safety, health, and economic benefits of fluoridation. (Mertz
A, Allukian M. – J Mass Dent Soc. 2014 Summer;63(2):32-6)
https://www.ncbi.nlm.nih.gov/pubmed/24635653
Does fluoride in drinking water delay tooth eruption?
RESULTS: By age 7, almost all permanent first molars had erupted. The adjusted mean number of erupted permanent first molars per child were 3.81, 3.67, and 3.92 in areas with
<0.3, 0.3-<0.7, and 0.7-1.2 ppm of fluoride, respectively. The adjusted caries attack rate in the first permanent molars among 5- to 17-year-old children was 93, 81, and 78 per 1,000 surfaces in fluoride deficient, suboptimal, and optimally fluoridated areas, respectively (P < 0.0001). This pattern of higher first molar attack rate among children in the fluoride-deficient communities was also observed in all erupted teeth.
CONCLUSION: Exposure to fluoride in drinking water did not delay the eruption of permanent teeth. The observed difference in dental caries experience among children exposed to different fluoride levels could not be explained by the timing of eruption of permanent teeth.
(Jolaoso IA, et al. – J Public Health Dent. 2014 Summer;74(3):241-7)
https://www.ncbi.nlm.nih.gov/pubmed/2442582828
Is fluoride a risk factor for bone cancer? Small area analysis of osteosarcoma
and Ewing sarcoma diagnosed among 0-49-year-olds in Great Britain, 1980-2005:
CONCLUSIONS: The findings from this study provide no evidence
that higher levels of fluoride (whether natural or artificial) in drinking
water in GB lead to greater risk of either osteosarcoma or Ewing sarcoma.
(Blakey K1, et al. – Int J Epidemiol. 2014 Feb;43(1):224-34)
https://www.ncbi.nlm.nih.gov/pubmed/2496284242
Eye cancer incidence in U.S. states and access to fluoridated water:
Environmental risk factors for uveal melanomas (cancer of the iris,
ciliary body, and choroid) have not been identified. To search for these,
we examined the correlation of age-adjusted eye cancer incidence rates,
a surrogate for uveal melanoma rates, in U.S. states with group level geographic
and demographic factors using multivariate linear regression. Incidence
rates for eye cancer were inversely correlated with the percentage of the
population receiving fluoridated water; that is, higher rates were found
in states with lower prevalences of fluoridation (P = 0.01). Fluoride is
known to inhibit the growth of microbial agents that cause choroiditis and
choroidal lesions in animals. We speculate that fluoridation protects against
choroidal melanoma by inhibiting microbial agents that cause choroiditis
and/or choroidal lesions in humans. (Schwartz GG – Cancer Epidemiol Biomarkers
Prev. 2014 Sep;23(9):1707-11)
https://www.ncbi.nlm.nih.gov/pubmed/2447054242
Effects of Life-long Fluoride Intake on Bone Measures of Adolescents:
A Prospective Cohort Study: The findings suggest that fluoride
exposures at the typical levels for most US adolescents in fluoridated areas
do not have significant effects on bone mineral measures. (Levy SM, et
al. – J Dent Res. 2014 Apr;93(4):353-9)
Discussion
https://www.ncbi.nlm.nih.gov/pubmed/24890821
Association of dental caries with socioeconomic status in relation to
different water fluoridation levels: CONCLUSIONS: This study
supported that water fluoridation could not only lead to a lower prevalence
of dental caries, but also help to reduce the effect of SES inequalities
on oral health. (Cho HJ, et al. – Community Dent Oral Epidemiol. 2014 Dec;42(6):536-42)
https://www.ncbi.nlm.nih.gov/pubmed/2482004949
Effectiveness of water fluoridation in caries reduction in a remote Indigenous
community in Far North Queensland: BACKGROUND: Children in remote
Indigenous communities in Australia have levels of dental caries much greater
than the national average. One such, the Northern Peninsula Area of Far
North Queensland (NPA), had an oral health survey conducted in 2004, shortly
before the introduction of fluoridated, reticular water. Children were again
surveyed in 2012, following five years exposure. CONCLUSIONS: There has
been considerable improvement in child dental health in the NPA over the
past 6-7 years. In light of continued poor diet and oral hygiene, water
fluoridation is the most likely explanation. The cost-effectiveness for
this small community remains an issue which, in the current climate of political
antagonism to water fluoridation in many quarters, requires continued study.
(Johnson NW, et al. – Aust Dent J. 2014 Sep;59(3):366-71)
https://www.ncbi.nlm.nih.gov/pubmed/24603270
An alternative marker for the effectiveness of water fluoridation: hospital
extraction rates for dental decay, a two-region study: OBJECTIVES:
To examine inpatient hospital episodes statistics for dental extractions
as an alternative population marker for the effectiveness of water fluoridation
by comparing hospital admissions between two major strategic health authority
(SHA) areas, the West Midlands SHA-largely fluoridated--and the North West
SHA--largely unfluoridated. METHOD: Hospital episodes statistics (HES) were
interrogated to provide data on admissions for simple and surgical dental
extractions, which had a primary diagnostic code of either dental caries
or diseases of pulp and periapical tissues for financial years 2006/7, 2007/8
and 2008/9. Data was aggregated by SHA area and quinary age group. Directly
standardised rates (DSR) of admissions purchased for each primary care trust
(PCT) were calculated and ranked by index of multiple deprivation (IMD).
RESULTS: A significant difference in DSRs of admission between PCTs in the
West Midlands and North West was observed (Mann-Whitney U test [p <0.0001])
irrespective of IMD ranking. The difference in rates between the two most
deprived PCTs was 27-fold. CONCLUSIONS: After ranking by IMD, DSRs of hospital
admissions for the extraction of decayed or pulpally/periapically involved
teeth is lower in areas with a fluoridated water supply. (Elmer TB, et
al. – Br Dent J. 2014 Mar;216(5):E10)
https://www.ncbi.nlm.nih.gov/pubmed/2442835050
Systemic effect of water fluoridation on dental caries prevalence:
CONCLUSIONS: While 6-year-old children who had not ingested fluoridated
water showed higher dft in the WF-ceased area than in the non-WF area, 11-year-old
children in the WF-ceased area who had ingested fluoridated water for approximately
4 years after birth showed significantly lower DMFT than those in the non-WF
area. This suggests that the systemic effect of fluoride intake through
water fluoridation could be important for the prevention of dental caries.
(Cho HJ, et al. – Community Dent Oral Epidemiol. 2014 Jan 16)
https://www.ncbi.nlm.nih.gov/pubmed/2430839595
Milk fluoridation for the prevention of dental caries: CONCLUSION:
These evaluations showed clearly that the optimal daily intake of fluoride
in milk is effective in preventing dental caries. The amount of fluoride
added to milk depends on background fluoride exposure and age of the children:
commonly in the range 0.5 to 1.0 mg per day. An advantage of the method
is that a precise amount of fluoride can be delivered under controlled conditions.
The cost of milk fluoridation programmes is low, about - 2 to 3 per child
per year. Fluoridation of milk can be recommended as a caries preventive
measure where the fluoride concentration in drinking water is suboptimal,
caries experience in children is significant, and there is an existing school
milk programme. (Beneczy J et al. – Acta Med Acad. 2013 Nov;42(2):156-67)
https://www.ncbi.nlm.nih.gov/pubmed/23889610
Factors associated with surface-level caries incidence in children aged
9 to 13: the Iowa Fluoride Study: CONCLUSION: More frequent tooth
brushing was protective of sound surfaces, and fluoride in home tap water
was also protective, but significantly more so for adolescents in low-income
families. (Broffitt B, et al. – J Public Health Dent. 2013 Fall;73(4):304-10
https://www.ncbi.nlm.nih.gov/pubmed/23556545
Reduced adhesion of oral bacteria on hydroxyapatite by fluoride treatment:
The mechanisms of action of fluoride have been discussed controversially
for decades. The cavity-preventive effect for teeth is often traced back
to effects on demineralization. However, an effect on bacterial adhesion
was indicated by indirect macroscopic studies. To characterize adhesion
on fluoridated samples on a single bacterial level, we used force spectroscopy
with bacterial probes to measure adhesion forces directly. We tested the
adhesion of Streptococcus mutans , Streptococcus oralis , and Staphylococcus
carnosus on smooth, high-density hydroxyapatite surfaces, pristine and after
treatment with fluoride solution. All bacteria species exhibit lower adhesion
forces after fluoride treatment of the surfaces. These findings suggest
that the decrease of adhesion properties is a further key factor for the
cariostatic effect of fluoride besides the decrease of demineralization.
(Loskill P, et al. – Langmuir. 2013 May 7;29(18):5528-33
https://www.ncbi.nlm.nih.gov/pubmed/2430839393
Water fluoridation and oral health: CONCLUSION: Water fluoridation
is an effective safe means of preventing dental caries, reaching all populations,
irrespective of the presence of other dental services. Regular monitoring
of dental caries and fluorosis is essential particularly with the lifelong
challenge which dental caries presents. (Harding MA, O'Mullane DM – Acta
Med Acad. 2013 Nov;42(2):131-9)
https://www.ncbi.nlm.nih.gov/pubmed/2429381010
The economic value of Quebec's water fluoridation program: RESULTS:
The analyses showed the water fluoridation program was cost-effective even
with a conservatively estimated 1 % reduction in dental caries. The benefit-cost
ratio indicated that, at an expected average effectiveness of 30 % caries
reduction, one dollar invested in the program saved $71.05-$82.83 per Quebec's
inhabitant in dental costs (in 2010) or more than $560 million for the State
and taxpayers. CONCLUSION: The results showed that the drinking-water fluoridation
program produced substantial savings. Public health decision-makers could
develop economic arguments to support wide deployment of this population-based
intervention whose efficacy and safety have been demonstrated and acknowledged.
(Tchouaket E, et al. – Z Gesundh Wiss. 2013;21:523-533)
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3837190/0/
The economic
value of Quebec's water fluoridation program: Aim: Dental caries
is a major public health problem worldwide, with very significant deleterious
consequences for many people. The available data are alarming in Canada
and the province of Quebec. The water fluoridation program has been shown
to be the most effective means of preventing caries and reducing oral health
inequalities. This article analyzes the cost-effectiveness of Quebec's water
fluoridation program to provide decision-makers with economic information
for assessing its usefulness. Conclusion: The results showed that the drinking-water
fluoridation program produced substantial savings. Public health decision-makers
could develop economic arguments to support wide deployment of this population-based
intervention whose efficacy and safety have been demonstrated and acknowledged.
(Eric Tchouaket, et al. – Z Gesundh Wiss. 2013; 21(6): 523-533)
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3840655/
Dental caries
in 14- and 15-year-olds in New South Wales, Australia: Teenagers
living in fluoridated areas of NSW had lower mean DMFT rates (DMFT 1.1 versus
1.7, Table 5) and a higher percentage of children who had never experienced
decay (56.0% versus 45.0%) than children in un-fluoridated areas. (John
Skinner, et al. – BMC Public Health. 2013; 13: 1060)
https://www.ncbi.nlm.nih.gov/pubmed/24084670
Estimated Drinking Water Fluoride Exposure and Risk of Hip Fracture.
A Cohort Study: Overall, we found no association between chronic
fluoride exposure and the occurrence of hip fracture. The risk estimates
did not change in analyses restricted to only low-trauma osteoporotic hip
fractures. Chronic fluoride exposure from drinking water does not seem to
have any important effects on the risk of hip fracture, in the investigated
exposure range. (Nesman P, et al. – J Dent Res. 2013 Oct 1)
https://www.ncbi.nlm.nih.gov/pubmed/23763747 -
Free Article
Understanding Public Decision-Making on Community Water Fluoridation
(CWF): Understanding public concern and building from common ground
when engaging the public can effectively build trust. 'Trust is difficult
to build once a CWF campaign is already underway,' adds Dr. Swan. The report
found that although public trust in scientific and medical organizations
cannot be relied on, people's trust in their own practitioners remained
high. 'So, discussing CWF with your patients may help build public support
for CWF.' (J Can Dent Assoc. 2013 May;79:d77)
Related:
Effectiveness of Population-Based Interventions to Promote Oral Health
https://www.ncbi.nlm.nih.gov/pubmed/23456704
Effects of Fluoridated Drinking Water on Dental Caries in Australian
Adults: The study shows that Australian adults with more than 75% lifetime
exposure to water fluoridation have significantly reduced caries experience
when compared with those with less than a 25% lifetime exposure. This reduction
has occurred in adult Australians born in both the pre- and post-fluoridation
generation. The significance of this is that the introduction of water fluoridation
to a community will benefit all residents, not only those who grow up drinking
fluoridated water. (Slade GD, et al. – J Dent Res. 2013 Mar 1)
https://www.ncbi.nlm.nih.gov/pubmed/23550501
Fluoridation and dental caries severity in young children treated under
general anaesthesia: an analysis of treatment records in a 10-year case
series: CONCLUSIONS: Children with severe dental caries had statistically
significantly lower numbers of lesions if they lived in a fluoridated area.
The lower treatment need in such high-risk children has important implications
for publicly-funded dental care.. (Kamel MS, et al. – Community Dent Health.
2013 Mar;30(1):15-8)
https://www.ncbi.nlm.nih.gov/pubmed/23327241
Water fluoridation and the association of sugar-sweetened beverage consumption
and dental caries in Australian children: Consumption of sugar-sweetened
beverages should be considered a major risk factor for dental caries. However,
increased exposure to fluoridated public water helped ameliorate the association
between SSB consumption and dental decay. These results reconfirm the benefits
of community water fluoridation for oral health. (Mullen J, et al. – Am
J Public Health. 2013 Mar;103(3):494-500)
https://www.ncbi.nlm.nih.gov/pubmed/23488212
Caries status in 16 year-olds with varying exposure to water fluoridation
in Ireland: RESULTS: With both systems of measurement, significantly
lower caries levels were found in those children with the greatest exposure
to fluoridated water when compared to those with the least exposure.
CONCLUSIONS: The survey provides further evidence of the effectiveness in
reducing dental caries experience up to 16 years of age. The extra intricacies
involved in using the Percentage Lifetime Exposure method did not provide
much more information when compared to the simpler Estimated Fluoridation
Status method. . (Armfield JM, et al. – Community Dent Health. 2012 Dec;29(4):293-6)
https://www.ncbi.nlm.nih.gov/pubmed/22910620
-
Free Article
Prevalence of dental caries and dental fluorosis
among 12 and 15 years old school children in relation to fluoride concentration
in drinking water in an endemic fluoride belt of Andhra Pradesh: CONCLUSION:
There was a negative correlation between dental caries and fluoride concentration
for the entire study population. However, in high fluoride areas, there
was a positive correlation between fluoride concentration and dental caries.
Water defluoridation on an urgent basis is a priority here than water fluoridation,
because the prevalence and severity of dental flurorosis is very high.
According to our study, an optimum range of fluoride concentration in
this area that offered maximum protection against dental caries with minimal
risk for esthetically significant fluorosis, was 0.6 - 1.3 PPM. This is
very close to the optimal fluoride concentration of 0.6 - 1.2 PPM, suggested
by Bureau of Indian standards. (Shekar C, et al. – Indian J Public Health.
2012 Apr-Jun;56(2):122-8)
https://www.ncbi.nlm.nih.gov/pubmed/23272895
-
Free Article
The association between social deprivation and
the prevalence and severity of dental caries and fluorosis in populations
with and without water fluoridation: CONCLUSIONS: Water fluoridation
appears to reduce the social class gradient between deprivation and caries
experience when considering caries into dentine. However, this was associated
with an increased risk of developing mild fluorosis. The use of intra-oral
cameras and remote scoring of photographs for caries demonstrated good potential
for blinded scoring. (McGrady MG, et al. – BMC Public Health. 2012 Dec 28;12:1122)
https://www.ncbi.nlm.nih.gov/pubmed/23252588
Decline in dental caries among 12-year-old children in Brazil, 1980-2005:
CONCLUSIONS: Data showed a significant decrease in dental caries across
the entire country, with an average reduction of 25% occurring every 5 years.
General trends indicated that a reduction in DMFT index values occurred
over time, that a further reduction in DMFT index values occurred when a
municipality fluoridated its water supply, and mean DMFT index values were
lower in larger than in smaller municipalities. (Lauris JR, et al. – Int
Dent J. 2012 Dec;62(6):308-14)
https://www.ncbi.nlm.nih.gov/pubmed/23192605
-
Free Article
Fluorides - mode of action and recommendations for
use: Various authors have shown that the caries decline in the industrialized
countries during recent decades is based on the use of fluorides, of which
local fluoride application in the form of fluoridated toothpastes is of
primary importance. The caries-protective potential of fluorapatite is quite
low; in contrast, dissolved fluorides in the vicinity of enamel are effective
both in promoting remineralization and inhibiting demineralization. Considering
the fact that the caries decline occurred at the same time that local fluoridation
measures became widely used, the conclusion seems justified that regular
application of F⁻ can inhibit caries. (Lussi A, et al. – Schweiz Monatsschr
Zahnmed. 2012;122(11):1030-42)
https://www.ncbi.nlm.nih.gov/pubmed/22998306
Effectiveness of water fluoridation in caries prevention: CONCLUSIONS:
Fewer studies have been published recently. More of these have investigated
effect at the multi-community, state or even national level. The dmf/DMF
index remains the most widely used measure of effect. % CR were lower in
recent studies, and the 'halo' effect was discussed frequently. Nevertheless,
reductions were still substantial. Statistical control for confounding factors
is now routine, although the effect on per cent reductions tended to be
small. Further thought is needed about the purpose of evaluation and whether
measures of effect and study design are appropriate for that purpose. (Rugg-Gunn
AJ & Do L. – Community Dent Oral Epidemiol. 2012 Oct;40 Suppl 2:55-64)
https://www.ncbi.nlm.nih.gov/pubmed/22554069
A model to determine the economic viability of water fluoridation:
CONCLUSIONS: This model confirmed that water fluoridation is an economically
viable option to prevent dental caries in South African communities, as
well as conclusions over the last 10 years that water fluoridation leads
to significant cost savings and remains a cost-effective measure for reducing
dental caries, even when the caries-preventive effectiveness is modest.
(Kroon J & van Wyk PJ. – J Public Health Dent. 2012 Fall;72(4):327-33)
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3134728/
Battle renewed
over value of fluoridation: Linking the decision made by the United
States Department of Health and Human Services to lower the recommended
level of fluoride added to drinking water to the effectiveness of water
fluoridation is inaccurate. This decision was based on studies showing that
the levels previously accepted in the US presented a risk of dental fluorosis
that was deemed unacceptable for infant formula reconstituted with tap water.
The change was a dosage adjustment, not a retreat from water fluoridation.
The reference to the balance of protection and risk confirms that the decision
had nothing to do with 'bone effects' and everything to do with fluorosis.
There is no evidence that exposure to fluoride from water fluoridation leads
to bone abnormalities of any kind. (MacGregor, R. – CMAJ. 2011 July 12;
183(10): 1173. )
https://www.ncbi.nlm.nih.gov/pubmed/22189446
Fluoride in drinking water and osteosarcoma incidence rates in the continental
United States among children and adolescents: CONCLUSION: Our ecological
analysis suggests that the water fluoridation status in the continental
U.S. has no influence on osteosarcoma incidence rates during childhood and
adolescence. (Levy M, Leclerc BS. – Cancer Epidemiol. 2012 Apr;36(2):e83-8)
Drinking water fluoridation in CanadaReview and synthesis of
published literature, April 2011. Main findings may be summarized
as follows:
- Evidence for the effectiveness of drinking water fluoridation
in the prevention of dental caries in Canada exists. The strongest
evidence is from the original trials (e.g., Brantford-Sarnia-Stratford)
in the 1940s through 1960s. These original trials were impressive
for their adherence to a rigorous research protocol.
- Since the 1970s, research on drinking water fluoridation has
been complicated by the widespread availability of other sources
of fluoride, most notably fluoride toothpaste. As such, more recent
evidence on fluoridation is weaker than the earliest findings, though
on balance it supports more than it refutes the effectiveness of
the intervention.
- Existing research consistently shows an association between
exposure to drinking water fluoridation and increased risk of dental
fluorosis. Case studies of fluorosis in communities with high levels
of fluoride in drinking water illustrate the critical importance
of monitoring fluoride concentrations, particularly in rural areas
with weaker infrastructure.
- Although there is some indication that exposure to fluoridation
may have some benefit for bone density, on balance there is no clear
evidence for an association between drinking water fluoridation
and health outcomes other than dental outcomes.
- To conduct research on the health impact of drinking water fluoridation,
it is essential to have accurate information on exposure, including
a) length of residence in the community; and b) use of other sources
of fluoride. This has implications for oral health surveillance
across multiple Canadian jurisdictions.
- Although resistance to fluoridation is sometimes thought to
be a recent phenomenon, well-defined opposition to fluoridation
has in fact existed as long as fluoridation itself.
- Many arguments have been put forth by those opposed to fluoridation,
ranging from the relatively innocuous 'it's not effective' to the
more apocryphal 'communist plot' and 'aluminum company conspiracy'.
Part of the power of the anti-fluoride movement is that some of
the arguments - e.g., potential harm to the environment and aquatic
life - cross ideological lines and have proponents in both the political
right and left.
- We identified a large amount of material on local circumstances
surrounding plebiscites or referenda. While this information may
be helpful for communities undergoing a vote, it is important to
recognize that fluoridation plebiscites are more likely to fail
than to pass, which reflects characteristics of fluoridation and
characteristics of plebiscites.
- Contrasting with the failure of most fluoridation plebiscites
is the observation, from public opinion polls, that a majority of
Canadians are in favour of, or at least not opposed to, fluoridation.
This suggests that anti-fluoridationists are over-represented among
voters at plebiscites, and it speaks to the success of the anti-fluoridationists
in persuading otherwise undecided or non-voters to vote no.
- From an ethical point of view, drawing on principles of beneficence,
autonomy, and truthfulness, the controversy over fluoridation may
be un-resolvable. (McLaren L. & McIntyre L., )
Calgary's
City Council voted 10-3 to remove fluoride from the city's drinking
water on Feb. 8, 2011. Dr. McLaren has initiated a
study
to follow results of this decision on the city's youth - results
are expected (from one source) in spring, 2015.
https://www.ncbi.nlm.nih.gov/pubmed/21479915
Drinking water fluoridation and osteosarcoma incidence on the island
of Ireland: The results of this study do not support the hypothesis
that osteosarcoma incidence in the island of Ireland is significantly related
to public water fluoridation. However, this conclusion must be qualified,
in view of the relative rarity of the cancer and the correspondingly wide
confidence intervals of the relative risk estimates. (Comber H, et al. – Cancer Causes Control. 2011 Jun;22(6):919-24)
https://www.ncbi.nlm.nih.gov/pubmed/22161414
Fluoride supplements (tablets, drops, lozenges or chewing gums) for preventing
dental caries in children: BACKGROUND: Dietary fluoride supplements
were first introduced to provide systemic fluoride in areas where water
fluoridation is not available. Since 1990, the use of fluoride supplements
in caries prevention has been re-evaluated in several countries. MAIN
RESULTS: We included 11 studies in the review involving 7196 children.In
permanent teeth, when fluoride supplements were compared with no fluoride
supplement (three studies), the use of fluoride supplements was associated
with a 24% (95% confidence interval (CI) 16 to 33%) reduction in decayed,
missing and filled surfaces (D(M)FS). AUTHORS' CONCLUSIONS: This review
suggests that the use of fluoride supplements is associated with a reduction
in caries increment when compared with no fluoride supplement in permanent
teeth. The effect of fluoride supplements was unclear on deciduous teeth.
When compared with the administration of topical fluorides, no differential
effect was observed. We rated 10 trials as being at unclear risk of bias
and one at high risk of bias, and therefore the trials provide weak evidence
about the efficacy of fluoride supplements. (Tubert-Jeannin S, et al. – Cochrane Database Syst Rev. 2011 Dec 7;12:CD007592.)
https://www.ncbi.nlm.nih.gov/pubmed/21799046
(copy
of the paper)
An Assessment of Bone Fluoride and Osteosarcoma:
No significant association between bone fluoride levels and osteosarcoma
risk was detected in our case-control study, based on controls with other
tumor diagnoses.
(Kim FM, et al. – J Dent Res. 2011 Oct;90(10):1171-1176.
Epub 2011 Jul 28)
https://www.ncbi.nlm.nih.gov/pubmed/21599939
-
Free Article
Validation of a multifactorial risk factor
model used for predicting future caries risk with Nevada adolescents:
{logistic regression analysis indicated that youth living in non-fluoridated
areas of Nevada had greater odds of developing tooth decay than those who
lived in the county with fluoridated water - RJ}
(Ditmyer MM, et
al. – BMC Oral Health. 2011; 11: 18. Published online 2011 May 20)
Related
article:
https://www.ncbi.nlm.nih.gov/pubmed/20857070
-
Free Article
https://www.ncbi.nlm.nih.gov/pubmed/21466692
Inequalities of caries experience in Nevada youth expressed by DMFT index
vs. Significant Caries Index (SiC) over time: At the community level,
action should focus on retaining and expanding the community fluoridation
program as an effective preventive measure. (Ditmyer MM, et al. – BMC Oral Health. 2011 Apr 5;11:12)
https://www.ncbi.nlm.nih.gov/pubmed/21426851
Dental caries in children: a comparison of one non-fluoridated and two
fluoridated communities in NSW: The caries prevalence in the permanent
dentition of Lithgow {non-fluoridated} children was significantly higher
than that in children living in the fluoridated towns of Bathurst and Orange
{fluoridated}. No significant differences were observed in the estimates
for primary teeth.
CONCLUSION: Although the mean levels of dental caries
in schoolchildren in Lithgow were low, oral health inequalities exist between
children residing in non-fluoridated Lithgow and the fluoridated locations
of Orange and Bathurst. The local council decided that Lithgow will have
fluoridated water by December 2010. (Arora A & Evans RW – N S W Public
Health Bull. 2010 Nov-Dec;21(11-12):257-62)
https://www.ncbi.nlm.nih.gov/pubmed/20857070
-
Free Article
Fluoride: its role in dentistry: In
spite of decades of research on fluoride and the recognition of its role
as the cornerstone of dental caries reduction in the last fifty years, questions
still arise on its use at community, self-applied and professional application
levels. Which method of fluoride delivery should be used? How and when should
it be used? How can its benefits be maximized and still reduce the risks
associated with its use? These are only some of the challenging questions
facing us daily. The aim of this paper is to present scientific background
to understand the importance of each method of fluoride use considering
the current caries epidemiological scenario, and to discuss how individual
or combined methods can be used based on the best evidence available.
(Tenuta LM, Cury JA – Braz Oral Res. 2010;24 Suppl 1:9-17) {a very
good summary of the role of the fluoride ion, saliva, and oral ecology on
the process of tooth decay - RJ}
http://www.publichealthreports.org/archives/issuecontents.cfm?Volume=125&Issue=5 (requires
subscription)
Geographic Variation in Medicaid Claims for Dental Procedures
in New York State: Role of Fluoridation Under Contemporary Conditions:
Results. Compared with the predominantly fluoridated counties, the mean
number of restorative, endodontic, and extraction procedures per recipient
was 33.4% higher in less fluoridated counties. Conclusions. We found
that the mean number of claims for caries related services for children
in the NYS Medicaid program was correlated with the extent of fluoridation
in a county. These annual decreases in claims per recipient, when applied
to lifetime exposure of the whole population, have large societal benefits.
These findings, when added to the already existing weight of evidence, have
implications for promoting policies at the federal and state levels to strengthen
the fluoridation program. (Kumar, JV, et al. – Public Health Reports, September
- October 2010, Volume 125 p647)
https://www.ncbi.nlm.nih.gov/pubmed/20873281
Community Effectiveness of Public Water Fluoridation in Reducing Children's
Dental Disease: Results. Children from every age group had greater caries
prevalence and more caries experience in areas with negligible fluoride
concentrations in the water (<0.3 parts per million [ppm]) than in optimally
fluoridated areas (>0.7 ppm). Conclusions. This study demonstrates
the continued community effectiveness of water fluoridation and provides
support for the extension of this important oral health intervention to
populations currently without access to fluoridated water. (Armfield, JM
– Public Health Reports, September - October 2010, Volume 125 p655-664)
https://www.ncbi.nlm.nih.gov/pubmed/20545833
What we know and do not know about fluoride: Summary: There is much
that we know about fluoride as it relates to human health in general and
dental health in particular. Some of the information that is known concerning
water fluoridation and dental fluorosis is listed. What we do not know about
fluoride is discussed in more detail, namely the efficacy of lower levels
of fluoride in drinking water, the effect of discontinuing fluoride in drinking
water in the absence of additional preventive measures, the prevalence of
fluorosis and whether or not this presents a cosmetic problem. Other issues
discussed include the actual amount of fluoride ingested from all sources,
whether low-fluoride dentifrices are as efficacious as conventional dentifrices
in caries protection and reducing enamel fluorosis, the role of socioeconomic
factors in determining caries prevalence, and the effects of bottled water
use on caries prevalence in fluoridated communities. (Newbrun E. – J Public
Health Dent. 2010 Jun 2. [Epub ahead of print])
https://www.ncbi.nlm.nih.gov/pubmed/20415910
The impact of changing dental needs on cost savings from fluoridation:
CONCLUSION: Community water fluoridation remains a cost-effective preventive
measure in Australia. (Campain AC, et al. – Aust Dent J. 2010 Mar;55(1):37-44)
https://www.ncbi.nlm.nih.gov/pubmed/20406153
Drinking water fluoridation in South East Queensland: a cost-effectiveness
evaluation: CONCLUSION: Fluoridation remains still a very cost-effective
measure for reducing dental decay. (Ciketic S, et al. – Health Promot J
Austr. 2010 Apr;21(1):51-6)
https://www.ncbi.nlm.nih.gov/pubmed/20415937
Water fluoridation in the Blue Mountains reduces risk of tooth decay:
CONCLUSIONS: Tooth decay reduction observed in the Blue Mountains corresponds
to high rates reported elsewhere and demonstrates the substantial benefits
of water fluoridation. (Evans RW, et al. – Aust Dent J. 2009 Dec;54(4):368-73)
https://www.ncbi.nlm.nih.gov/pubmed/20858781
The long-term effects of water fluoridation on the human skeleton:
Municipal water fluoridation has notably reduced the incidence of dental
caries and is widely considered a public health success. However, ingested
fluoride is sequestered into bone, as well as teeth, and data on the long-term
effect of exposure to these very low doses of fluoride remain inconclusive.
Epidemiological studies suggest that effects of fluoride on bone are minimal.
We hypothesized that the direct measurement of bone tissue from individuals
residing in municipalities with and without fluoridated water would reveal
a relationship between fluoride content and structural or mechanical properties
of bone. However, consonant with the epidemiological data, only a weak relationship
among fluoride exposure, accumulated fluoride, and the physical characteristics
of bone was observed. Analysis of our data suggests that the variability
in heterogenous urban populations may be too high for the effects, if any,
of low-level fluoride administration on skeletal tissue to be discerned.
(Chachra D, et al. – J Dent Res. 2010 Nov;89(11):1219-23)
https://www.ncbi.nlm.nih.gov/pubmed/20640347
-
Free Article
Epidemiology of fluorosis and dental caries according
to different types of water supplies: Conclusions: Only the schoolchildren
in the WTS {fluoridated water} group presented a DMFT index {the total number
of teeth with caries experience, including decayed teeth} below 3, probably
because of the better water fluoridation, demonstrating the efficacy of
this method; thus, this preventive measure should be recommended for our
population. (Franzolin Sde O, et al. – Cien Saude Colet. 2010 Jun;15 Suppl
1:1841-7)
https://www.ncbi.nlm.nih.gov/pubmed/20858781
The long-term effects of water fluoridation on the human skeleton:
Abstract - Municipal water fluoridation has notably reduced the incidence of dental caries and is widely considered a public health success. However, ingested fluoride is sequestered into bone, as well as teeth, and data on the long-term effect of exposure to these very low doses of fluoride remain inconclusive. Epidemiological studies suggest that effects of fluoride on bone are minimal. We hypothesized that the direct measurement of bone tissue from individuals residing in municipalities with and without fluoridated water would reveal a relationship between fluoride content and structural or mechanical properties of bone. However, consonant with the epidemiological data, only a weak relationship among fluoride exposure, accumulated fluoride, and the physical characteristics of bone was observed. Analysis of our data suggests that the variability in heterogenous urban populations may be too high for the effects, if any, of low-level fluoride administration on skeletal tissue to be discerned.
(Chachra D, Limeback H, Willett TL, Grynpas MD – J Dent Res. 2010 Nov;89(11):1219-23)
https://www.ncbi.nlm.nih.gov/pubmed/20724674
The association between community water fluoridation (CWF) and adult
tooth loss: CONCLUSIONS: This study suggests that the benefits of CWF
may be larger than previously believed and that CWF has a lasting improvement
in racial/ethnic and economic disparities in oral health. (Neidell M, et
al. – Am J Public Health. 2010 Oct;100(10):1980-5)
https://www.ncbi.nlm.nih.gov/pubmed/21067620
-
Free Article
A case-control study of determinants for high
and low dental caries prevalence in Nevada youth: Community water fluoridation
has been documented as the most cost-effective, equitable, and safe community-based
approach to improving oral health. Participants living in areas without
community water fluoridation in Nevada were almost 2 times more likely to
present with higher DMFT indices. The benefits of water fluoridation are
proportionally higher for people who do not have regular access to other
sources of fluoride. Therefore, dental professionals should counsel patients
living in non-fluoridated geographic areas on the importance of using other
sources of fluoride. It is of special significance that several futile attempts
have been made in Nevada to introduce community water fluoridation to other
counties, such as Washoe County, which comprises around 15% of the population.
(Ditmyer M, et al. – BMC Oral Health. 2010 Nov 11;10:24)
https://www.ncbi.nlm.nih.gov/pubmed/19772843
Water fluoridation: AIM: This was to present
a summary of the evidence from systematic reviews of the effectiveness and
safety of water fluoridation
RESULTS: Of the 59 publications identified,
3 systematic reviews and 3 guidelines were included in this review. While
the reviews themselves were of good methodological quality, the studies
included in the reviews were generally of moderate to low quality. The results
of the three reviews showed that water fluoridation is effective at reducing
caries in children and adults. With the exception of dental fluorosis, no
association between adverse effects and water fluoridation has been established.
Water fluoridation reduces caries for all social classes, and there is some
evidence that it may reduce the oral health gap between social classes.
CONCLUSION: Water fluoridation, where technically feasible and culturally
acceptable, remains a relevant and valid choice as a population measure
for the prevention of dental caries. (Parnell C, et al. – Eur Arch Paediatr
Dent. 2009 Sep;10(3):141-8)
Related Article Community Water Fluoridation:
An Evidence Review, 2012, Campos-Outcalt, et al.
https://www.ncbi.nlm.nih.gov/pubmed/19571049
The Association Between Enamel Fluorosis and Dental Caries in U.S. Schoolchildren:
Conclusion. This study's findings suggest that molars with fluorosis are
more resistant to caries than are molars without fluorosis.
Clinical
Implications. The results highlight the need for those considering policies
regarding reduction in fluoride exposure to take into consideration the
caries-preventive benefits associated with milder forms of enamel fluorosis.
(Hiroko, I, et al. – J Am Dent Assoc, Vol 140, No 7, 855-862, 2009)
https://www.ncbi.nlm.nih.gov/pubmed/192369133
Appetitive-based learning in rats: lack of effect of chronic exposure
to fluoride: CONCLUSION: Chronic ingestion of fluoride {by rats} at
levels up to 230 times more than that experienced by humans whose main source
of fluoride is fluoridated water had no significant effect on appetitive-based
learning.(Whitford, GM, et al. – Neurotoxicol Teratol. 2009 Jul-Aug;31(4):210-5)
https://www.ncbi.nlm.nih.gov/pubmed/196949322
Risk perception and water fluoridation support and opposition in
Australia: Objectives: A considerable body of evidence confirms that
water fluoridation effectively reduces the community incidence of dental
caries with minimal side effects. However, proposals to introduce this widely
endorsed public-health measure are often perceived as controversial, and
public opinion frequently plays a role in the outcome. Despite this, the
public's perception of risk associated with water fluoridation has not been
well researched and remains poorly understood. Our objectives were to determine
whether risk perceptions reflecting various "outrage" factors
are associated with water fluoridation support and opposition. Conclusion:
Outrage factors are important aspects of the public's perception of risk
in relation to water fluoridation. Given that water fluoridation appears
to be a low-risk, high-outrage controversy, efforts to mitigate the level
of public outrage, rather than continuing to deny possible hazards, may
offer a worthwhile strategy in gaining public acceptance for the extension
of water fluoridation. (Armfield, JM and Akers, HF – J Public Health Dent.
2009 Aug 20)
https://www.ncbi.nlm.nih.gov/pubmed/19797552
Assessing a potential risk factor for enamel fluorosis: a preliminary
evaluation of fluoride content in infant formulas: Some infants aged
between birth and 6 months who consume powdered and liquid concentrate formulas
reconstituted with water containing 1.0 part per million fluoride likely
will exceed the upper tolerable limit of fluoride. CONCLUSIONS: When powdered
or liquid concentrate infant formulas are the primary source of nutrition,
some infants are likely to exceed the recommended fluoride upper limit if
the formula is reconstituted with water containing 1.0 ppm fluoride. On
the other hand, when the fluoride concentration in water used to reconstitute
infant formulas is below 0.4 ppm, it is likely that infants between 6 and
12 months of age will be exposed to fluoride at levels below IOM's recommended
adequate intake level. (Siew, C et al. – J Am Dent Assoc. 2009 Oct;140(10):1228-36)
https://www.ncbi.nlm.nih.gov/pubmed/19947132
A controlled study of risk factors for enamel hypoplasia in the permanent
dentition: PURPOSE: The purpose of this study was to investigate risk
factors for enamel hypoplasia (EH) and enamel opacity (EO) in the permanent
teeth of healthy schoolchildren from a nonfluoridated community in Australia.
CONCLUSIONS: Children with low socioeconomic status, histories of respiratory
or chickenpox infections, exposure to cigarette-smoking, urinary tract infections,
otitis, and use of adult toothpaste are predisposed to enamel hypoplasia.
By contrast, drinking optimally fluoridated water at 0 to 3 years old reduces
the risk for enamel opacities. (Ford, D et al. – Pediatr Dent. 2009 Sep-Oct;31(5):382-8)
https://www.ncbi.nlm.nih.gov/pubmed/19820737
Evidence that fluoride in the infant formula causes enamel fluorosis
weak: CONCLUSIONS: Infant formula consumption may be associated with
an increased risk of developing at least some detectable level of enamel
fluorosis, but this depends on the level of fluoride in the water
supply. The evidence that the fluoride in the infant formula caused
enamel fluorosis was weak, as other mechanisms could explain the
observed association. (Edwards, M –
Evid Based Dent. 2009;10(3):73)
https://www.ncbi.nlm.nih.gov/pubmed/19630837
Association of natural
fluoride in community water supplies with dental health of children in remote
indigenous communities - implications for policy: OBJECTIVE:
To map the geographic distribution of fluoride in water supplies and child
dental caries in remote Indigenous communities of the Northern Territory
(NT). To examine the association between fluoride levels, household and
community factors, access to services and child dental caries in these communities
and to model the impact on the caries experience of children of introducing
water fluoridation. CONCLUSIONS AND IMPLICATIONS: Introduction of
fluoridation of water supplies into communities with inadequate natural
fluoride is a vital measure for improving the dental health of children
living in remote NT communities. (Bailie, RS, et al. – Aust N Z J Public
Health. 2009 Jun;33(3):205-11)
https://www.ncbi.nlm.nih.gov/pubmed/19627654
Water fluoridation in Canada: past and present: Water fluoridation
remains a contentious issue in Canada and many communities choose not to
fluoridate their water supply. As of 2007, 45.1% of the Canadian population
had access to fluoridated water supplies. The main arguments for and against
fluoridation have changed very little over the years, with supporters (including
the World Health Organization and Health Canada) citing evidence that shows
fluoridation as a safe and effective method of caries prevention, while
detractors cite high costs and potential health risks. This article provides
an historical overview and a current snapshot of water fluoridation in Canada.
It concludes that the ultimate advantage of fluoridation is that it helps
everyone in a community, regardless of socioeconomic status. (Rabb-Waytowich
D – J Can Dent Assoc. 2009 Jul;75(6):451-4)
https://www.ncbi.nlm.nih.gov/pubmed/18515990
Effects of long-term fluoride in drinking water on risks of hip fracture
of the elderly: an ecologic study based on database of hospitalization episodes,
OBJECTIVES: Fluoridation of drinking water is known to decrease dental caries,
particularly in children. However, the effects of fluoridated water on bone
over several decades are still in controversy. To assess the risk of hip
fracture related to water fluoridation, we evaluated the hip fracture-related
hospitalizations of the elderly between a fluoridated city and non-fluoridated
cities in Korea.
CONCLUSIONS: We cannot conclude that fluoridation of
drinking water increases the risk of hip fracture in the elderly. (Park
EY, et al. – J Prev Med Public Health. 2008 May;41(3):147-52)
https://www.ncbi.nlm.nih.gov/pubmed/19320724
Prevalence and extent of dental caries, dental fluorosis, and developmental
enamel defects in Lithuanian teenage populations with different fluoride
exposures: The aim of this study was to describe the pattern of dental
caries, dental fluorosis, and developmental defects of non-fluoride origin
in Lithuanian children born and raised in regions with 1.1 ppm (1.1 mg/l
F) and 0.3 ppm (0.3 mg/l F) water fluoride levels, respectively. All permanent
surfaces/teeth of 300 teenagers were examined for dental caries, dental
fluorosis, and non-fluoride developmental defects. The caries prevalence
of the study population was 100%. The mean number of decayed surfaces (DS)
differed only slightly and statistically insignificantly between the '1.1
ppm fluoride' and '0.3 ppm fluoride' groups (19.6 and 18.1, respectively).
However, a greater number of inactive lesions and fewer fillings were found
in the '1.1 ppm fluoride' group than in the '0.3 ppm fluoride' group (mean
difference 1.18 and -2.80, respectively). The prevalence of dental fluorosis
was 45% and 21%, respectively; the prevalence of non-fluoride opacities
was 8% and 19%, respectively; and the prevalence of hypoplasia was 12% and
16%, respectively, in the '1.1 ppm fluoride' and '0.3 ppm fluoride' groups.
Higher caries levels were noted in children with no fluorosis compared to
those with fluorosis recorded (mean DS difference, 3.43). The results lend
support to the hypothesis that the presence of fluoride in the oral environment
promotes lesion arrest rather than inhibiting the initiation of new lesions.
(Machiulskiene V, et al. – Eur J Oral Sci. 2009 Apr;117(2):154-60)
https://www.ncbi.nlm.nih.gov/pubmed/19839282
Public opinions on community water fluoridation: BACKGROUND: Community
water fluoridation (CWF) is currently experiencing social resistance in
Canada. Petitions have been publicly registered, municipal plebiscites have
occurred, and media attention is growing... RESULTS: Approximately
1 in 2 Canadian adults surveyed knew about CWF. Of these, 80% understood
its intended use, approximately 60% believed that it was both safe and effective,
and 62% supported the idea of having fluoride added to their local drinking
water. Those with greater incomes [OR=1.4; p<0.001] and education [OR=1.6;
p<0.001] were more likely to know about CWF. Those with greater incomes
[OR=1.3; p<0.03] and those who visited the dentist more frequently [OR=1.8;
p<0.002] were more likely to support CWF, and those with children [OR=0.5;
p<0.02], those who accessed dental care using public insurance [OR=0.2;
p<0.03], and those who avoided fluoride [OR=0.04; p<0.001] were less
likely to support CWF. CONCLUSION: It appears that Canadians still
support CWF. In moving forward, policy leaders will need to attend to two
distinct challenges: the influence of anti-fluoride sentiment, and the potential
risks created by avoiding fluoride. (Quionez CR, Locker D. – Can J Public
Health. 2009 Mar-Apr;100(2):96-100) {Ironically,
the segment of the population most at risk for dental disease and the group
most likely to benefit from water fluoridation policies is often the group
most opposed to the practice. RJ}
https://www.ncbi.nlm.nih.gov/pubmed/19281105
The global increase in dental caries. A pending public health crisis:
A current review of the available epidemiological data from many countries
clearly indicates that there is a marked increase in the prevalence of dental
caries. This global increase in dental caries prevalence affects children
as well as adults, primary as well as permanent teeth, and coronal as well
as root surfaces. This increase in dental caries signals a pending public
health crisis. Although there are differences of opinion regarding the cause
of this global dental caries increase, the remedy is well known: a return
to the public health strategies that were so successful in the past, a renewed
campaign for water fluoridation, topical fluoride application, the use of
fluoride rinses, a return to school oral health educational programs, an
emphasis on proper tooth brushing with a fluoride dentifrice, as well as
flossing, a proper diet and regular dental office visits. (Bagramian RA,
et al. – Am J Dent. 2009 Feb;22(1):3-8)
https://www.ncbi.nlm.nih.gov/pubmed/18584000
A systematic review of the efficacy and safety of fluoridation: SCOPE
AND PURPOSE: The systematic review was commissioned by the Australian National
Health and Medical Research Council (NHMRC) to evaluate the scientific literature
relating to the health effects of fluoride and fluoridation. The systematic
review's research questions relate to the caries-reducing benefits and associated
potential health risks of providing fluoride systemically (via addition
to water, milk and salt) and the use of topical fluoride agents, such as
toothpaste, gel, varnish and mouthrinse. - RECOMMENDATIONS: Fluoridation
of drinking water remains the most effective and socially equitable
means of achieving community-wide exposure to the caries prevention
effects of fluoride. It is recommended
https://www.ncbi.nlm.nih.gov/pubmed/18422709
Lifetime fluoridation exposure and dental caries experience in a military
population: OBJECTIVES: To determine whether exposure to fluoride in
drinking water is associated with caries experience in Australian Defence
Force (ADF) personnel.
CONCLUSIONS: Degree of lifetime exposure to fluoridated
drinking water was inversely associated with DMFT in a dose-response manner
among this adult military population. (Mahoney, G, et al. – Community Dent
Oral Epidemiol. 2008 Dec;36(6):485-92) {Translation - the greater the exposure
to fluoridated drinking water the lower the rate of DMFT (the number of
decayed, missing and filled teeth) - RJ.}
https://www.ncbi.nlm.nih.gov/pubmed/18514162
Pharmacokinetics of ingested fluoride: lack of effect of chemical compound,
CONCLUSIONS: Considered together with published reports, the present findings
support the conclusion that the major features of fluoride metabolism are
not affected differently by the chemical compounds commonly used to fluoridate
water nor are they affected by whether the fluoride is present naturally
or added artificially. (Whitford, GM, et al. – Arch Oral Biol. 2008 Nov;53(11):1037-41)
https://www.ncbi.nlm.nih.gov/pubmed/18694870
Is Water Fluoridation Still Necessary?
Water fluoridation has been promoted in many countries as an organized
community effort to control dental caries. With the availability of
fluorides targeted at individuals and the decline in dental caries, the
need for fluoridation has been questioned. Recent reports show that
water fluoridation, a community-level intervention, continues to be an
efficient method for the delivery of fluoride in many countries. The
advantages include its ability to deliver low levels of fluoride to
saliva frequently, with high reach, at low cost, and with substantial
cost savings. Water fluoridation has the potential to reduce oral health
disparities by creating a healthy environment. Other forms of fluoride,
such as fluoride toothpaste, and clinical interventions complement
dental caries control strategies. (Kumar, JV – Adv Dent Res 20:8-12, July,
2008)
https://www.ncbi.nlm.nih.gov/pubmed/18329450
Fluorides in dental public health programs: The use of fluorides
in dental public health programs has a long history. With the availability
of fluoridation and other forms of fluorides, dental caries have declined
dramatically in the United States. This article reviews some of the ways
fluorides are used in public health programs and discusses issues related
to their effectiveness, cost, and policy. (Kumar JV, Moss ME – Dent Clin
North Am. 2008 Apr;52(2):387-401, vii. )
https://www.ncbi.nlm.nih.gov/pubmed/18333872
European citizens' opinions on water fluoridation: OBJECTIVES: To
understand European citizens' opinions on water fluoridation, as part of
research on their attitudes to the tensions between private and public interest.
CONCLUSIONS: While the vast majority of people opposed water fluoridation,
this may be indicative of shifts away from public support of population
interventions towards private interventions, as well as reduced trust in
public agencies. Thus if research were to demonstrate more clear benefits
of water fluoridation over and above that which can be achieved by use of
fluoride toothpaste, then the public may become more supportive. However,
lobby groups are likely to remain influential. (Griffin, M, et al. – Community
Dent Oral Epidemiol. 2008 Apr;36(2):95-102)
https://www.ncbi.nlm.nih.gov/pubmed/18319589
Prospective study of the association between fluoride intake and dental
fluorosis in permanent teeth: CONCLUSIONS: There was no difference between
children with and without fluorosis in the permanent central incisors and
first molars regarding fluoride intake. However, this study has limitations
that must be recognized: fluoride intake was only measured once, and there
were no children in the sample with severe degrees of dental fluorosis.
(Martins, CC, et al. – Caries Res. 2008;42(2):125-33)
https://www.ncbi.nlm.nih.gov/pubmed/18515990
Effects of long-term fluoride in drinking water on risks of hip fracture
of the elderly: an ecologic study based on database of hospitalization episodes:
CONCLUSIONS: We cannot conclude that fluoridation of drinking water increases
the risk of hip fracture in the elderly. (Park EY, et al. – J Prev Med Public
Health. 2008 May;41(3):147-52)
https://www.ncbi.nlm.nih.gov/pubmed/18661604
Dental caries of lifetime residents in Baixo Guandu, Brazil, fluoridated
since 1953--a brief communication: The addition of fluoride to public
water supplies was an important ally in the improvement of the oral health
of Baixo Guandu inhabitants. (Saliba, NA, et al. – J Public Health Dent.
2008 Spring;68(2):119-21)
https://www.ncbi.nlm.nih.gov/pubmed/18259663
The ethical dilemma of water fluoridation: The aim of this study
is to analyze some of the ethical arguments for and against water fluoridation
and to determine if empirical data allow to decide if there are correct
policies from a bioethical perspective. Autonomy, compulsory medication
(mass medication), precautionary principle, justice in health care and ethics
of protection are discussed. It is concluded that fluoridation is beneficial
and that there is no ethical reason to oppose it, based on a specific kind
of ethics developed to analyze and clarify complex public health issues.
(Mendoza, VC – Rev Med Chil. 2007 Nov;135(11):1487-93. )
https://www.ncbi.nlm.nih.gov/pubmed/18087993
A comparison of dental treatment utilization and costs by HMO members
living in fluoridated and nonfluoridated areas:
OBJECTIVES: To compare
dental treatment experiences and costs in members of a health maintenance
organization (HMO) in areas with and without community water fluoridation.
RESULTS: Community water fluoridation was associated with reduced total
and restorative costs among members with one or more visits, but the magnitude
and direction of the effect varied with locale and age and the effects were
generally small. In two locales, the cost of restorations was higher in
nonfluoridated areas in young people (<age 18) and older adults (>age
58). In younger adults, the opposite effect was observed. The impact of
fluoridation may be attenuated by higher use of preventive procedures, in
particular supplemental fluorides, in the nonfluoridated areas. (Maupom
G, et al. – J Public Health Dent. 2007 Fall;67(4):224-33)
https://www.ncbi.nlm.nih.gov/pubmed/17891121
Fluoride prevents caries among adults of all ages: CONCLUSIONS: To
date, no systematic reviews have found fluoride to be effective in preventing
dental caries in adults. The objective of this meta-analysis was to examine
the effectiveness of self- and professionally applied fluoride and water
fluoridation among adults. ...These findings suggest that fluoride
is effective in preventing caries in adults of all ages. (Yeung, CA – Evid
Based Dent. 2007;8(3):72-3)
http://ndt.oxfordjournals.org/content/22/10/2763.long
Effects
of fluoridation of community water supplies for people with chronic kidney
disease:
- There is no evidence that consumption of optimally fluoridated
drinking water increases the risk of developing CKD, although only limited
studies addressing this issue are available.
- There is no evidence that
consumption of optimally fluoridated drinking water poses any health risks
for people with CKD, although only limited studies addressing this issue
are available
- There is limited evidence that people with stage 4 or
5 CKD who ingest substances with a high concentration of fluoride may be
at risk of fluorosis.
(Ludlow M, et al. – Nephrol Dial Transplant. 2007
Oct;22(10):2763-7
https://www.ncbi.nlm.nih.gov/pubmed/17452559
Effectiveness of fluoride in preventing caries in adults: These findings
suggest that fluoride {topical and water fluoridation} prevents caries among
adults of all ages. (Griffin, SO, et al. – J Dent Res. 2007 May;86(5):410-5)
https://www.ncbi.nlm.nih.gov/pubmed/17333303
Community water fluoridation and caries prevention: a critical review:
The aim of this paper was to critically review the current role of community
water fluoridation in preventing dental caries. Original articles and reviews
published in English language from January 2001 to June 2006 were selected
through MEDLINE database. Other sources were taken from the references of
the selected papers. For the past 50 years community water fluoridation
has been considered the milestone of caries prevention and as one of the
major public health measures of the 20th century. However, it is now accepted
that the primary cariostatic action of fluoride occurs after tooth eruption.
Moreover, the caries reduction directly attributable to water fluoridation
have declined in the last decades as the use of topical fluoride had become
more widespread, whereas enamel fluorosis has been reported as an emerging
problem in fluoridated areas. Several studies conducted in fluoridated and
nonfluoridated communities suggested that this method of delivering fluoride
may be unnecessary for caries prevention, particularly in the industrialized
countries where the caries level has became low. Although water fluoridation
may still be a relevant public health measure in poor and disadvantaged
populations, the use of topical fluoride offers an optimal opportunity to
prevent caries among people living in both industrialized and developing
countries. (Pizzo, G, et al. – Clin Oral Investig. 2007 Sep;11(3):189-93)
https://www.ncbi.nlm.nih.gov/pubmed/17167257
Effects of water fluoride exposure at crown completion and maturation
on caries of permanent first molars: Pre-eruptive fluoride exposure
has been shown to be important for caries prevention. This paper aimed to
determine the relative effects of water fluoride exposure during crown completion
(CC) and maturation on caries experience in first permanent molars... In
conclusion a high exposure at CC was important for caries prevention irrespective
of the effect of exposure at maturation and post-eruption. The strongest
caries-preventive effect was produced by a high exposure at CC supplemented
by a high exposure at maturation and/or post-eruption, but the latter two
phases could not produce a significant caries-preventive effect on their
own. Since most of the caries occurred on pit and fissure surfaces, the
findings relate to this class of lesion. (Singh KA, et al. – Caries Res.
2007;41(1):34-42)
https://www.ncbi.nlm.nih.gov/pubmed/16774166
Fluoride: a controversy revisited: The purpose of this article is
to provide a review of the small but loud debate that has surrounded fluoride
over the past 50 years. The benefits of fluoridation and its effect on public
health are well known throughout the dental community. What is far less
well known are the objections from people--in the tradition of the old amalgam
and radiograph radiation debates-who feel that fluoride has adverse effects
serious enough to warrant a cessation of its use. This article will present
both sides of the issue, not to influence the reader, but to allow the reader
to realize that this issue exists and to understand what the key arguments
are. (Ananian, A. et al. – N Y State Dent J. 2006 Apr-May;72(3):14-8)
https://www.ncbi.nlm.nih.gov/pubmed/16683594
Reexamination of hexafluorosilicate hydrolysis by 19F NMR and pH measurement:
The dissociation of hexafluorosilicate has been reinvestigated due to recent
suggestions that fluorosilicate intermediates may be present in appreciable
concentrations in drinking water... No intermediates
were observable at 10(-5) M concentrations under excess fluoride forcing
conditions over the pH range of 3.5-5. ...The buffer capacity of all
of these systems was found to be insufficient to prevent acidic shifts in
pH when hexafluorosilicate was added. The pH change is sufficient explanation
for the observed inhibition of acetylcholinesterase that was previously
attributed to hexafluorosilicate hydrolysis intermediates. (Finney, WF,
et al. – Environ Sci Technol. 2006 Apr 15;40(8):2572-7)
https://www.ncbi.nlm.nih.gov/pubmed/17063019
Fluoride intake from food and liquid in Japanese children living in two areas with different fluoride concentrations in the water supply: The mean DMFT in the moderate fluoride area (MFA) was significantly lower than that in the low fluoride area (LFA). The severest grade of dental fluorosis observed was 'very mild' according to Dean's fluorosis index in both areas. The total daily fluoride intakes were 0.0252-0.0254 mg F/kg/day in the MFA [average 0.56 ppm] and 0.0126-0.0144 mg F/kg/day in the LFA [0.04 - 0.13 ppm]. Differences in the fluoride concentration of drinking water in this study were reflected in the fluoride intake from the diet in a typical Japanese diet. (Nohno K,
et al. – Caries Res. 2006;40(6):487-93)
https://www.ncbi.nlm.nih.gov/pubmed/16555718
Dental caries and enamel fluorosis among the fluoridated population in
the Republic of Ireland and non fluoridated population in Northern Ireland
in 2002: CONCLUSIONS: In 2002 apart from 8-year-olds, caries levels
were lower amongst children resident in fluoridated communities in RoI than
amongst corresponding age groups in non-fluoridated NI. Caries has declined
in fluoridated and non fluoridated groups in both jurisdictions since the
early 1960s. In RoI fluorosis levels were higher amongst lifetime residents
of fluoridated communities and have increased since 1984. (Whelton, H,
et al. – Community Dent Health. 2006 Mar;23(1):37-43)
https://www.ncbi.nlm.nih.gov/pubmed/16263039
-
Free Full Article
Costs and savings associated with community
water fluoridation programs in Colorado: CONCLUSION: Colorado realizes
significant annual savings from CWFPs; additional savings and reductions
in morbidity could be achieved if fluoridation programs were implemented
in other areas. (O'Connell, JM, et al. – Prev Chronic Dis. 2005 Nov;2 Spec
no:A06)
https://www.ncbi.nlm.nih.gov/pubmed/16393670
Blood Lead Concentrations in Children and Method of Water Fluoridation
in the United States, 1988-1994: Given these findings, our analyses,
though not definitive, do not support concerns that silicofluorides in community
water systems cause higher PbB concentrations in children. Current
evidence does not provide a basis for changing water fluoridation practices,
which have a clear public health benefit. (Macek, MD, et al. – Environmental
Health Perspectives Volume 114, Number 1, January 2006)
https://www.ncbi.nlm.nih.gov/pubmed/16246928
Bioavailability of fluoride in drinking water: a human experimental study:
It has been suggested that systemic fluoride absorption from drinking
water may be influenced by the type of fluoride compound in the water and
by water hardness. Using a human double-blind cross-over trial, we conducted
this study to measure c(max), T(max), and Area Under the Curve (AUC) for
plasma F concentration against time, following the ingestion of naturally
fluoridated hard and soft waters, artificially fluoridated hard and soft
waters, and a reference water. Mean AUC over 0 to 8 hours was 1330, 1440,
1679, 1566, and 1328 ng F.min.mL(-1) for naturally fluoridated soft, naturally
fluoridated hard, artificially fluoridated soft, artificially fluoridated
hard, and reference waters, respectively, with no statistically significant
differences among waters for AUC, c(max), or T(max). Any differences in
fluoride bioavailability between drinking waters in which fluoride is present
naturally or added artificially, or the waters are hard or soft, were small
compared with large within- and between-subject variations in F absorption.
(Maguire, A, et al. – J Dent Res. 2005 Nov;84(11):989-93)
https://www.ncbi.nlm.nih.gov/pubmed/16183366
Position of the American Dietetic Association: the impact of fluoride
on health, The American Dietetic Association reaffirms that fluoride
is an important element for all mineralized tissues in the body. Appropriate
fluoride exposure and usage is beneficial to bone and tooth integrity and,
as such, has an important, positive impact on oral health as well as general
health throughout life. The American Dietetic Association strongly reaffirms
its endorsement of the appropriate use of systemic and topical fluorides,
including water fluoridation, at appropriate levels as an important public
health measure throughout the life span. (Palmer, C, et al. – J Am Diet
Assoc. 2005 Oct;105(10):1620-8)
http://jn.nutrition.org/content/135/9/2247.full
Elevated Serum
Fluoride Concentrations in Women Are Not Related to Fractures and Bone Mineral
Density - Serum fluoride concentrations were not related to incident
osteoporotic fractures with 4 y of observation. Serum fluoride concentrations
were not associated with BMD or osteoporotic fractures among female residents
of communities with water fluoride concentrations of 52.6 or 210.4 ml/L. (Sowers
M, et al. – J. Nutr. 135:2247-2252, September 2005)
Effective use of fluorides for the prevention of dental caries in the 21st century
The WHO approach:
Effective use of fluorides for the prevention of dental caries in the 21st century: the WHO approach
Such reviews concluded that water fluoridation and use of fluoride toothpastes and mouthrinses significantly reduce the prevalence of dental caries. WHO recommends for public health that every effort must be made to develop affordable fluoridated toothpastes for use in developing countries. Water fluoridation, where technically feasible and culturally acceptable, has substantial advantages in public health; alternatively, fluoridation of salt and milk fluoridation schemes may be considered for prevention of dental caries. (Poul Erik Petersen & Michael A. Lennon – Community Dent Oral Epidemiol 2004)
https://www.ncbi.nlm.nih.gov/pubmed/15541159
Relative effects of pre- and post-eruption water fluoride on caries experience
by surface type of permanent first molars: CONCLUSIONS: Pre-eruption
exposure {to fluoridated water} was important for a caries preventive
effect on first permanent molars in children 6-15 years old since post-eruption
exposure alone could not lower caries levels significantly. (Singh,
KA, Spencer, AJ – Community Dent Oral Epidemiol. 2004 Dec;32(6):435-46)
https://www.ncbi.nlm.nih.gov/pubmed/15475904
Epidemiological studies of tooth wear and dental erosion in 14-year-old
children in North West England. Part 1: The relationship with water
fluoridation and social deprivation.
CONCLUSION: Children in non-fluoridated
districts are 1.5 times more likely to have smooth surface wear compared
with children in fluoridated districts. Fluoridation and use of fluoridated
toothpaste twice a day provide added protection from dental erosion. The
risk of tooth wear is greater with increasing affluence. (Bardsley, PF,
et al. – Br Dent J. 2004 Oct 9;197(7):413-6; discussion 399)
https://www.ncbi.nlm.nih.gov/pubmed/15341615
Effective use of fluorides for the prevention of dental caries in
the 21st century: the WHO approach: Research on the oral health effects
of fluoride started around 100 years ago; the focus has been on the link
between water and fluorides and dental caries and fluorosis, topical fluoride
applications, fluoride toothpastes, and salt and milk fluoridation. Most
recently, efforts have been made to summarize the extensive database through
systematic reviews. Such reviews concluded that water fluoridation and use
of fluoride toothpastes and mouthrinses significantly reduce the prevalence
of dental caries. (Petersen PE, Lennon MA – Community Dent Oral Epidemiol.
2004 Oct;32(5):319-21)
https://www.ncbi.nlm.nih.gov/pubmed/15337352
Relationship between fluorine in drinking water and dental health
of residents in some large cities in China: Our results, together with
the previous study, suggest that: (1) dental caries of the study population
can be reduced by drinking water fluoridation and that (2) other factors
such as economic level, weather, lifestyle, food habits, living condition,
etc., of a city can also affect the incidence of dental caries that cannot
be predicted by fluoridation alone. Research on the relation between index
of fluorosis (IF) and the fluorine concentration in drinking water for the
four high fluorine villages showed that the recommended concentration of
fluorine in drinking water can protect from dental fluorosis. (Wang, B,
et al. – Environ Int. 2004 Oct;30(8):1067-73)
https://www.ncbi.nlm.nih.gov/pubmed/15370629Caries
experience among schoolchildren in relation to community fluoridation status
and town size: {in Seo Paulo State, Brazil} Caries experience and prevalence
were significantly lower in fluoridated areas (1.9 DMFT, 2.1 dmft, 20% caries
free) than in non-fluoridated areas (2.4 DMFT, 2.4 dmft, 13% caries free). The
results suggest that water fluoridation is an essential public health measure
and that town size may affect caries distribution in the Southeast area
of Seo Paulo State. (Tagliaferro EP, et al. – Acta Odontol Scand. 2004 Jun;62(3):124-8)
https://www.ncbi.nlm.nih.gov/pubmed/15180079
Caries prevalence in a rural Chilean community after cessation of a powdered
milk fluoridation program: CONCLUSIONS: Termination of the powdered
milk fluoridation scheme resulted in a deterioration of the dental health
of children. After three years, dental caries prevalence was higher than
that reached at the end of the scheme and equivalent to that of the control
community without fluoride exposure. These results emphasize the need to
establish and maintain an alternative mechanism of community-based fluoridation
of proven effectiveness for the prevention of dental caries in communities
where water fluoridation is not available. (Marieo RJ, et al. – J
Public Health Dent. 2004 Spring;64(2):101-5)
https://www.ncbi.nlm.nih.gov/pubmed/15107774
Fluoride toxicity: CONCLUSIONS: Many years have passed since domestic
water fluoridation was adopted to reduce the incidence of caries in developed
countries; however, since there is an additional dose of fluorides ingested
with foods and drinks prepared with such waters, the problem has emerged
of possible adverse effects on health associated to them, so that in some
countries fluorine integrator selling is allowed only with preventive medical
prescription. ...At encephalic level, then, high doses of fluorine
cause the onset of neurological symptoms and of a decreased spontaneous
motor activity due to a reduction in the number of nicotinic acetylcholine
receptors. Nevertheless, epidemiological studies about fluoride toxicity
have established that such oligoelement may be safely used at odontoiatric
dosages. (Giachini M, Pierleoni F – Minerva Stomatol. 2004 Apr;53(4):171-7)
https://www.ncbi.nlm.nih.gov/pubmed/15346876
Water fluoridation and dental caries in 5- and 12-year-old children from
Canterbury and Wellington: Multivariable analysis confirmed the independent
association between water fluoridation and better dental health. CONCLUSIONS:
This results of this study show children living in a fluoridated area to
have significantly better oral health compared to those not in a fluoridated
area. These differences are greater for Maori and Pacific children and children
of low socio-economic status. (Lee M, Dennison PJ – N Z Dent J. 2004
Mar;100(1):10-5)
https://www.ncbi.nlm.nih.gov/pubmed/15067887
History of fluoride prevention: successes and problems (literature
review): Recent scientific views, however, confirmed a weak pre-, and
peri-eruptive, as well as a strong posteruptive effect of systemically applied
fluorides. In countries where caries prevalence is high, but the majority
of the population cannot afford fluoridated toothpastes due to low socio-economic
conditions, the introduction and extension of salt fluoridation to the whole
population is well founded and recommended from a public health view. (Beneczy
J, Marthaler TM – Fogorv Sz. 2004 Feb;97(1):3-10)
https://www.ncbi.nlm.nih.gov/pubmed/14631907
Optimal fluoride level in drinking water and public health: Water
fluoridation is a safe, efficient, and well-proven way of preventing dental
decay in the community. In countries such as Israel, where dental care is
not covered by the national insurance law, this has an important role in
reducing social inequalities in health care. For toddlers and children,
water fluoridation is the only way of promoting dental health without a
need for regular visits to dental clinics, and without regard to parent
awareness and motivation. The other methods of fluoride supplementation
do not succeed in reaching the level of safety and cost-efficiency of water
fluoridation, and their use is successful only among upper socio-economic
classes. Water fluoridation has been defined by the US CDC as one of the
main achievements in health care during the 20th century. In spite of the
legal difficulties raised by various activist groups, the use of water fluoridation
is growing steadily among developed as well as third world countries. The
Israeli bylaw of national water fluoridation that is in effect will enable
the safe improvement of the overall dental health status of the population
at an extremely low cost. (Karsenty E, et al. – Harefuah. 2003 Nov;142(11):754-8,
806)
https://www.ncbi.nlm.nih.gov/pubmed/15645934
Successes and drawbacks in the caries-preventive use of fluorides--lessons
to be learnt from history: Water fluoridation was the first breakthrough
in the practice of preventive cariology on a community level and has remained
one of the cornerstones of prevention in dentistry. The concepts regarding
the mechanisms of the caries-inhibitory effect, however, have changed in
several respects. Today there is general agreement that topical effects
on the erupted enamel are most important. The contention that there is no
pre-eruptive effect whatsoever has created confusion; there is in fact evidence
for a minor pre-eruptive protective effect. Around 1980 many experts believed
that fluorides should not be used in high concentrations, for instance above
those in dentifrices, because this could block remineralisation in the body
of pre-cavity lesions. However, it is now known that such undesirable effects
are negligible or non-existent. (Marthaler TM – Oral Health Prev Dent. 2003;1(2):129-40)
https://www.ncbi.nlm.nih.gov/pubmed/12734021
An update on fluorides and fluorosis: Decisions concerning use
of fluoride in its many forms for caries prevention are more complicated
now than in the past because of the need to balance these benefits with
the risks of dental fluorosis. This article reviews pertinent literature
concerning dental fluorosis (definition, appearance, prevalence), pre- and
post-eruptive use of fluoride, esthetic perceptions of dental fluorosis,
fluoride levels of beverages and foods, the Iowa Fluoride Study, and the
U.S. Centers for Disease Control and Prevention's "Recommendations
for Using Fluoride to Prevent and Control Dental Caries in the United States."
Water fluoridation and use of fluoride dentifrice are the most efficient
and cost-effective ways to prevent dental caries; other modalities should
be targeted toward high-risk individuals. (Levy SM – Dent Clin North Am.
2003 Apr;47(2):225-43)
https://www.ncbi.nlm.nih.gov/pubmed/12739679
History of water fluoridation: Analyses showed that maximum protection
against caries is obtained when teeth erupt into an environment with low
concentrations of ionic fluoride. The similarity in caries reductions obtained
in water fluoridation studies and long-term studies with topically administered
fluoride regimens, including fluoride-containing dentifrices, indicates
that the pre-eruptive effect of fluoride is of borderline significance relative
to the more significant post-eruptive effect. It has taken a long time to
show that water fluoridation and topical fluoride programs were thus important
measures for the control of caries at the community level.
(Kargul B,
et al. – J Clin Pediatr Dent. 2003 Spring;27(3):213-7)
https://www.ncbi.nlm.nih.gov/pubmed/12699229
Current and future role of fluoride in nutrition: Fluoride continues
to be the cornerstone of dental caries prevention in North America and throughout
the world, and there are a variety of sources of fluoride that may contribute
to the dietary intakes of fluoride. Although the severe effect of chronic
exposures to high levels of fluoride--skeletal fluorosis--is extremely rare
in North America, dental fluorosis has become more prevalent. To address
the increase in dental fluorosis prevalence, recommendations have been made
to reduce fluoride ingestion early in life. These recommendations have included
the introduction of lower concentration fluoride dentifrice for use by young
children, labeling of the fluoride concentration of bottled water, and revised
fluoride supplement guidelines to reduce or eliminate their use. Because
our knowledge is incomplete regarding the amount, duration, and timing of
fluoride ingestion that can result in dental fluorosis, however, further
research is clearly needed before definitive recommendations can be made
regarding the use of fluorides, including recommended intakes of fluoride
in the diet. (Warren JJ, Levy SM – Dent Clin North Am. 2003 Apr;47(2):225-43)
https://www.ncbi.nlm.nih.gov/pubmed/14595871
Decline in enamel hypoplasia in relation to fluoridation in Australians:
Enamel hypoplasias are thought to represent calcification disruption
indicative of metabolic stress during development. Hypoplasias of permanent
maxillary central incisors and mandibular canines have undergone a notable
reduction in frequency between Euro-Australian twins born around 1965 and
those born ca. 1990. Even when scored very liberally these linear defects
are 3.1-4.6 times as prevalent in the earlier Australians, and the discrepancy
is proportionately greater among strictly scored defects. Likely correlates
of this secular trend logically include reduced childhood fevers and clinical
intervention to reduce circum-natal stresses acting on cotwins. However,
fluoridation of metropolitan water has emerged as the statistically strongest
hypoplasia-preventing factor. (Corruccini RS, Townsend GC –
Am J Hum Biol. 2003 Nov-Dec;15(6):795-9
https://www.ncbi.nlm.nih.gov/pubmed/12508513
Fluoridation at fifty: what have we learned? The question posed
by the title of this article encompasses more than just the law and science
applied to fluoridation. A review of the history and present status of fluoridation
policy development and implementation makes it quickly apparent that the
lessons learned are applicable to a wide range of public health policy and
that the public health community needs to be very concerned about the status
and trends of legal precedent. Indeed, in the context of recent U. S. Supreme
Court decisions, the need for a comprehensive and coordinated effort
to educate the public, legislators, and jurists about the safety and efficacy
of community water fluoridation is clear. Two fundamental issues are
at the core of this article: (1) the use of science in formulating and defending
public health policy, and (2) how to connect scientific fact with the legal
process in connection with the actual circumstances regarding a community's
health status. The opening section of this article presents an analysis
of fluoridation's great success in preventing dental caries over the past
50 years, along with a discussion of current data scientifically demonstrating
that fluoride is safe when properly utilized. A second section provides
an overview of one state's legislative experience in mandating fluoridation
and the political challenges encountered. A final section discusses the
legal issues associated with fluoridation, including the bases of legal
challenges to public laws mandating it. (Pratt, E, et al. – J Law Med Ethics.
2002 Fall;30 (3 Suppl):117-21)
http://www.mrc.ac.uk/publications/browse/water-fluoridation-and-health/:
This report has considered the scope for further research that could help to inform risk management
decisions on water fluoridation. Our starting point was the knowledge base that is already established.
Much of this was recently reviewed in the report prepared by the York NHS CRD, and we have not
attempted to duplicate their work.We have, however, taken account of additional information (eg, on
pharmacology and toxicology) that did not fall within the scope of the York Review.
...There is almost universal agreement that tooth decay in children is related to social class.The majority of
the research conducted to date indicates that water fluoridation reduces dental caries inequalities
between high and low social class groups. Further studies are recommended that look at appropriate
measures of social inequalities related to water fluoridation, dental caries and fluorosis and possible
confounding factors.
Water Fluoridation and Health: (Medical Research Council working
group report, September 2002)
Free Article:
The York Review - A systematic review of public
water fluoridation: a commentary: The body of evidence available on
the efficacy and safety of water fluoridation was of lower quantity and
quality than had previously been reported.
> The best available evidence
(from studies that met inclusion criteria) suggests that fluoridation of
drinking water supplies reduces caries prevalence but is associated with
dental fluorosis.
> The balance of the evidence did not show an association
between any fractures and water fluoridation.
> No associations between
water fluoridation and human cancer were found. (Treasure, ET, et al. – British Dental Journal 192, 495 - 497 (2002))
another commentary
https://www.ncbi.nlm.nih.gov/pubmed/11918578
A blind caries and fluorosis prevalence study of school-children in naturally
fluoridated and nonfluoridated townships of Morayshire, Scotland: CONCLUSIONS:
Considerable caries benefit has accrued to those Morayshire rural children
who have received naturally fluoridated water (at 1 ppm) throughout their
lives, as compared to their socioeconomically similar, nonfluoridated rural
counterparts. Furthermore, in spite of all but two subjects claiming to
have brushed regularly with fluoridated dentifrice (and no evidence of the
availability of nonfluoridated toothpaste being purchasable in the five
townships), only borderline mild fluorosis disadvantages have been noted
clinically, and none by the subjects' own aesthetic perceptions. Finally,
no evidence was found to suggest any delay in permanent tooth eruption patterns
of the F subjects. It would seem appropriate therefore, that adjustment
of Scots' drinking waters' natural fluoride levels to 1 ppm should be pursued
to extend similar dental advantages to the vast majority of that population
(both young and old) which, it is well documented, has the worst dental
health of mainland UK. (Stephen, KW, et al. – Community Dent Oral Epidemiol.
2002 Feb;30(1):70-9)
https://www.ncbi.nlm.nih.gov/pubmed/11495635
-
Free Article
Association of Down's syndrome and water fluoride
level: a systematic review of the evidence: BACKGROUND: A review of
the safety and efficacy of drinking water fluoridation was commissioned
by the UK Department of Health to investigate whether the evidence supported
a beneficial effect of water fluoridation and whether there was any evidence
of adverse effects. Down's syndrome was one of the adverse effects reported.
The aim of this review is to examine the evidence for an association between
water fluoride level and Down's syndrome. - CONCLUSIONS: The evidence of
an association between water fluoride level and Down's syndrome incidence
is inconclusive. (Whiting P, et al. – BMC Public Health. 2001;1:6. Epub
2001 Jul 24)
https://www.ncbi.nlm.nih.gov/pubmed/11491235
Water fluoridation, osteoporosis, fractures--recent developments:
RESULTS: Thirty-three studies were identified. Adverse effects in animal feeding studies were only seen at doses much greater than those currently used in artificial water fluoridation. The majority of animal studies showed no effect or a beneficial effect of low fluoride doses. The results of ecological studies were conflicting. One of the two cohort studies showed an increase in fracture incidence at fluoride levels four times greater than optimal water fluoridation and the other showed no effect after 20 years' optimal fluoridation. The cross-sectional studies showed a favourable effect on bone mineral density. The clinical trials predominantly showed increased bone density in several sites associated with fluoride treatment of 9-22.6mg fluoride per day for one-four years.
CONCLUSION: These studies provide a substantial body of evidence that fluoride at up to 1ppm does not have an adverse effect on bone strength, bone mineral density or fracture incidence. (Demos LL,
et al. – Dent J. 2001 Jun;46(2):80-7)
http://www.nature.com/bdj/journal/v190/n1/abs/4800872a.html
Water
fluoridation: Community fluoridation - are there benefits? Objective:
To compare changes in dental health between non-fluoridated Stourbridge
and the towns of Dudley, Sedgeley and Coseley, Brierley Hill and Kingswinford,
and Halesowen that were artificially fluoridated in 1987. Conclusion: Drinking
water fluoridation is associated with an increase in the percentage of 5-year-old
children with no experience of tooth decay (Treasure, E – British Dental
Journal 190, 26 (2001)
https://www.ncbi.nlm.nih.gov/pubmed/11341339
Effect of long-term exposure to fluoride in drinking water on risks
of bone fractures: It is concluded that long-term fluoride exposure
from drinking water containing > or =4.32 ppm increases the risk of overall
fractures as well as hip fractures. Water fluoride levels at 1.00-1.06 ppm
decrease the risk of overall fractures relative to negligible fluoride in
water; however, there does not appear to be similar protective benefits
for the risk of hip fractures. (Li Y, et al. – J Bone Miner Res. 2001 May;16(5):932-9)
https://www.ncbi.nlm.nih.gov/pubmed/11021861
Free Article
Systematic review of water fluoridation:
OBJECTIVE: To review the safety and efficacy of fluoridation of drinking
water. DESIGN: Search of 25 electronic databases and world wide web. Relevant
journals hand searched; further information requested from authors. Inclusion
criteria were a predefined hierarchy of evidence and objectives. Study validity
was assessed with checklists. Two reviewers independently screened sources,
extracted data, and assessed validity.
RESULTS: 214 studies were included.
The quality of studies was low to moderate.
CONCLUSIONS: The evidence
of a beneficial reduction in caries should be considered together with
the increased prevalence of dental fluorosis. There was no clear evidence of
other potential adverse effects. (McDonagh MS, et al. – BMJ. 2000 Oct 7;321(7265):855-9)
http://www.cdc.gov/fluoridation/pdf/urbansky_schock.pdf
Can Fluoridation
Affect Lead(II) In Potable Water? Hexafluorosilicate and Fluoride Equilibria
In Aqueous Solutions: Conclusion - Recent reports on the possible effects
of water fluoridating agents, such as hexafluorosilicic acid, sodium hexafluorosilicate,
and sodium fluoride are inconsistent with accepted scientific knowledge,
and the authors fail to identify or account for these inconsistencies.
Many of the chemical assumptions are scientifically unjustified, and alternate
explanations (such as multiple routes of Pb exposure) have not been satisfactorily
addressed. At present, there is no evidence to suggest that the common
practice of fluoridating drinking water has any untoward health impacts
via effects on lead(II) when done properly under established guidelines
so as to maintain total water quality. Our conclusion supports both
EPA and PHS/CDC policies on water fluoridation. (Urbansky E.T. & Schock
M.R. – Intern. J . Environ. Studies, 2000, Vol. 57. pp. 597-637
https://www.ncbi.nlm.nih.gov/pubmed/11109211
The prevalence of dental caries and fluorosis in Japanese communities with up to 1.4 ppm of naturally occurring fluoride:
RESULTS: The prevalence of dental caries was inversely related and the prevalence of fluorosis was directly related to the concentration of fluoride in the drinking water. The mean DMFS in the communities with 0.8 to 1.4 ppm fluoride was 53.9 percent to 62.4 percent lower than that in communities with negligible amounts of fluoride. Multivariate analysis showed that water fluoride level was the strongest factor influencing DMFS scores. The prevalence of fluorosis ranged from 1.7 percent to 15.4 percent, and the increase in fluorosis with increasing fluoride exposure was limited entirely to the milder forms. (Tsutsui A,
et al. – J Public Health Dent. 2000 Summer;60(3):147-53)
https://www.ncbi.nlm.nih.gov/pubmed/11021862
Free Article
Community water fluoridation, bone mineral density,
and fractures: prospective study of effects in older women: CONCLUSIONS:
Long term exposure to fluoridated drinking water does not increase the risk
of fracture. (Phipps KR, et al.- BMJ. 2000 Oct 7;321(7265):860-4)
https://www.ncbi.nlm.nih.gov/pubmed/10860326
Free Article
Risk of enamel fluorosis in nonfluoridated and
optimally fluoridated populations: considerations for the dental professional:
CONCLUSIONS: Enamel fluorosis in the nonfluoridated study sample was attributed
to fluoride supplementation under the pre-1994 protocol and early toothbrushing
behaviors. Enamel fluorosis in the optimally fluoridated study sample was
attributed to early toothbrushing behaviors, inappropriate fluoride supplementation
and the use of infant formula in the form of a powdered concentrate. CLINICAL
IMPLICATIONS: By advising parents about the best early use of fluoride agents,
health professionals play an important role in reducing the prevalence of
clinically noticeable enamel fluorosis. (David G. Pendrys – J Am Dent Assoc.
2000 Jun;131(6):746-55.
https://www.ncbi.nlm.nih.gov/pubmed/10846267
Indigenous Australian dental health: a brief review of caries experience:
Abstract - The indigenous community in Australia is an at risk
population for oral diseases such as dental caries. The majority of communities
are isolated and dental services in these areas are limited. Oral hygiene
standards are poor and this combined with a diet rich in refined carbohydrates
has led to high incidences of dental caries. In addition, diabetes, which
is related to obesity (and a diet high in sugar and fat) has been linked
to increases in oral disease. Caries prevalence was found to be low in areas
where fluoridation levels in the water were high. The fact that the fluoride
supplementation appears to improve oral health to a significant degree suggests
that implementation of fluoride treatment programmes for school children
and, where viable, fluoridation of water sources would be appropriate. In
addition, dental education programmes should receive high priority. (Martin-Iverson
N, et al. – Aust Dent J. 2000 Mar;45(1):17-20.)
http://www.dentalwatch.org/fl/newbrun.html
Why We Have Not Changed Our Minds about the Safety and Efficacy of Water Fluoridation: A Response to John Colquhoun -
The opponents of fluoridation are a heterogeneous group and cannot easily be categorized by any single characteristic. Among their number are right-wing extremists, misguided environmentalists ("Greens"), chiropractors, persons concerned about the costs of fluoridation, food faddists, and antiscience "naturalists." Other opponents have emerged, including the self-proclaimed "neutrals" who try to portray an image of dispassionate open-mindedness but clearly have accepted the opposition's arguments irrespective of whether they have been adequately tested and answered [6,31,32]. Others have been described as the "born-again antifluoridationists" [33], who previously accepted the mainstream belief in the benefits of fluoridation but have experienced an epiphany so that the scales have fallen from their eyes and they have seen the light [2,34,35]. Clearly Colquhoun falls in this latter category. However, it is important to recognize that simply by claiming to be a former advocate and now clearly being a dedicated opponent of fluoridation in no way validates his judgment nor excuses his distortion of the literature.
(Ernest Newbrun, D.M.D., Ph.D.and Herschel Horowitz – Perspectives in Biology and Medicine 42:526-541, 1999)
https://www.ncbi.nlm.nih.gov/pubmed/10089229
The effect of fluoride treatment on bone mineral in rabbits: Fluoride
therapy has been used clinically for many years, but its use remains controversial
and many basic questions remain unanswered. Accordingly, this study returns
to an animal model to study the effects of high doses of fluoride on bone
mineral in rabbits. Twelve rabbits, aged 3(1/2) months at the start of the
study, received drinking water fluoridated at 100 ppm {note - that's
100 times the recommended level - rj} while their 12 control counterparts
drank distilled water. All rabbits were sacrificed after 6 months. Fluoride
was readily incorporated into femoral cortical bone (7473 +/- 966 ppm F
versus 1228 +/- 57 ppm in controls; P < 0.00005). Fluoride therapy led
to increased mineralization, as measured by density fractionation (P <
0.0005 for the distributions). The bone mineral itself was altered, with
a significant increase in the width of crystals (66.2 +/- 2.0 A versus 61.2
+/- 0.9 A; P < 0.01). The microhardness of both cortical and cancellous
bone in the femoral head of fluoride-treated rabbits was greater than that
in the controls (P < 0.05). The phosphate, calcium, and carbonate contents
in the bone was the same in both groups. Finally, fluoride administration
did not affect the architecture or connectivity of cancellous bone in the
femoral head. Previously published data [1] indicated that the mechanical
properties of bone were adversely affected; this suggests that the effect
of high doses of fluoride on the strength and stiffness of bone may be mediated
by its effect on bone mineral. (Chachra D, et al. – Calcif Tissue Int. 1999
Apr;64(4):345-51)
https://www.ncbi.nlm.nih.gov/pubmed/10077350
Drinking water fluoridation and bone: Accordingly, in most epidemiological
studies in humans bone mass was not altered by optimal drinking water fluoridation.
In contrast, studies on the effect on hip fracture rate gave conflicting
results ranging from an increased fracture incidence to no effect, and to
a decreased fracture rate. As only ecological studies have been performed,
they may be biased by unknown confounding factors -- the so-called ecological
fallacy. However, the combined results of these studies indicate that
any increase or decrease in fracture rate is likely to be small. It has
been calculated that appropriately designed cohort studies to solve the
problem require a sample size of >400,000 subjects. Such studies will
not be performed in the foreseeable future. Future investigations in humans
should, therefore, concentrate on the effect of long-term drinking water
fluoridation on bone fluoride content and bone strength. (Allolio B, Lehmann
R – Exp Clin Endocrinol Diabetes. 1999;107(1):12-20)
Achievements in Public Health, 1900-1999: Fluoridation of Drinking Water to Prevent Dental Caries
- Fluoridation of community drinking water is a major factor responsible for the decline in dental caries (tooth decay) during the second half of the 20th century. The history of water fluoridation is a classic example of clinical observation leading to epidemiologic investigation and community-based public health intervention. Although other fluoride-containing products are available, water fluoridation remains the most equitable and cost-effective method of delivering fluoride to all members of most communities, regardless of age, educational attainment, or income level.
(Reported by Div of Oral Health, National Center for Chronic Disease Prevention and Health Promotion, CDC., October, 1999)
https://www.ncbi.nlm.nih.gov/pubmed/9608443
Dental caries and dental fluorosis among schoolchildren who were lifelong residents of communities having either low or optimal levels of fluoride in drinking water: CONCLUSIONS:
Findings from the present study suggest that water fluoridation still is beneficial and that dental sealants can play a significant role in preventing dental caries. In addition, findings from this survey appear to support the premise that the difference in dental fluorosis prevalence between fluoridated and nonfluoridated communities has narrowed considerably in recent years. (Selwitz RH, et al., J Public Health Dent. 1998)
https://www.ncbi.nlm.nih.gov/pubmed/8897755
Fluoridation--the Israel
experience: There have been suggestions, mainly in the lay press, that
fluoridation might affect immunity. Careful examination of various studies
on fluoride and immune function do not support this suggestion. Whilst fluoride
at high concentrations can have inhibitory effects on lymphocyte and polymorphonuclear
leucocyte function, these concentrations are many times higher than levels
which would be expected from fluoridation. Fluoride can act as an immunological
adjuvant. There is no evidence of any deleterious effect on specific immunity
following fluoridation nor any confirmed reports of allergic reactions.
(Challacombe SJ – Community Dent Health. 1996 Sep;13 Suppl 2:69-71)
https://www.ncbi.nlm.nih.gov/pubmed/8897750
Fluoridation--the Israel
experience: Epidemiological studies have shown that 5- and 12-year-old
children living in fluoridated areas (in Israel) have considerably less
dental caries than those receiving unfluoridated water. (Kelman AM – Community
Dent Health. 1996 Sep;13 Suppl 2:42-6)
https://www.ncbi.nlm.nih.gov/pubmed/9034970
The effectiveness of
community water fluoridation in the United States: Grand Rapids, the
first city in the world to implement controlled water fluoridation, has
served as a model for thousands of other communities. Fluoridation is one
of the greatest public health and disease-preventive measures of all time.
Its advantages include effectiveness for all, ease of delivery, safety,
equity, and low cost. Today, nearly 56 percent of the US population lives
in fluoridated communities (62% of those on central water supplies). Previously
observed caries reductions of one-half to two-thirds are no longer attainable
in the United States because other fluoride methods and products have reduced
the caries prevalence in all areas, thus diluting the measurement of effectiveness,
and because benefits of fluoridation are dispersed in many ways to persons
in nonfluoridated areas. Water fluoridation itself, however, remains as
effective as it ever was among groups at high risk to dental caries. Contrary
to early beliefs that stressed the importance of preeruptive fluoride exposure,
fluoridation also provides an important source of topical fluoride and facilitates
remineralization. Although data on effectiveness and safety are compelling,
future progress of water fluoridation will be affected by economic, political,
and public perception factors. (Horowitz, HS – J Public Health Dent. 1996;56(5
Spec No):253-8)
https://www.ncbi.nlm.nih.gov/pubmed/8897754
Water fluoridation
and osteoporotic fracture: Data on the relationship between fluoride
intake and hip fracture risk at the individual level, and data relating
fluoridation to bone mineral density are required. Until these become available,
the burden of evidence suggesting that fluoridation might be a risk factor
for hip fracture is weak and not sufficient to retard the progress of the
water fluoridation programme.
(Hillier S, Inskip H, Coggon D, Cooper
C. – Community Dent Health. 1996 Sep;13 Suppl 2:63-8)
https://www.ncbi.nlm.nih.gov/pubmed/8897753
Cancer and fluoridation:
The present paper gives a brief overview of the evidence that fluoride in
drinking water has not been shown to cause an increase in the risk of developing
cancer and of the errors in the analyses that purport to show such an increase.
(Cook-Mozaffari P. – Community Dent Health. 1996 Sep;13 Suppl 2:56-62)
https://www.ncbi.nlm.nih.gov/pubmed/8897751
Thirty-eight years
of water fluoridation--the Singapore scenario: Singapore is the first
country in Asia to institute a comprehensive fluoridation programme which
covers 100 per cent of the population. The water was fluoridated at 0.7
ppm fluoride using sodium silicofluoride. The ten year study on the effects
of water fluoridation in Singapore showed a decrease in caries prevalence
in the children. In the permanent dentition the reduction was 52.3 per cent
for Chinese and 31 per cent for Malays in the 7 to 9 year old age group.
A similar trend was observed in the mixed dentition in which the decrease
was 32.5 per cent for Chinese and 30.6 per cent for Malays. Because of the
availability and use of other fluoride products, dental fluorosis was observed
in children in later years. Although the decline in dental caries after
10 years of water fluoridation was not comparable to those achieved in other
countries, this study further documents water fluoridation as the most cost-effective
public health measure for the prevention of dental caries. (Loh, T – Community
Dent Health. 1996 Sep;13 Suppl 2:47-50)
https://www.ncbi.nlm.nih.gov/pubmed/8741788
Free Article
Drinking water and cancer: Any and
all chemicals generated by human activity can and will find their way into
water supplies. The types and quantities of carcinogens present in drinking
water at the point of consumption will differ depending on whether they
result from contamination of the source water, arise as a consequence of
treatment processes, or enter as the water is conveyed to the user. Source-water
contaminants of concern include arsenic, asbestos, radon, agricultural chemicals,
and hazardous waste. Of these, the strongest evidence for a cancer risk
involves arsenic, which is linked to cancers of the liver, lung, bladder,
and kidney. The use of chlorine for water treatment to reduce the risk of
infectious disease may account for a substantial portion of the cancer risk
associated with drinking water. The by-products of chlorination are associated
with increased risk of bladder and rectal cancer, possibly accounting for
5000 cases of bladder cancer and 8000 cases of rectal cancer per year in
the United States. Fluoridation of water has received great scrutiny but
appears to pose little or no cancer risk. (Morris RD – Environ Health Perspect.
1995 Nov;103 Suppl 8:225-31)
https://www.ncbi.nlm.nih.gov/pubmed/7503344
Free Article
Fluoride exposure and childhood osteosarcoma:
a case-control study; CONCLUSIONS: Fluoride exposure does not increase
the risk of osteosarcoma and may be protective in males. The protective
effect may not be directly due to fluoride exposure but to other factors
associated with good dental hygiene. There is also biologic plausibility
for a protective effect. (Gelberg KH, et al. – Am J Public Health. 1995
Dec;85(12):1678-83)
https://www.ncbi.nlm.nih.gov/pubmed/7643331
Dental fluorosis and caries prevalence in children residing in communities with different levels of fluoride in the water: CONCLUSIONS: The ingestion of water containing 1 ppm or less fluoride during the time of tooth development may result in dental fluorosis, albeit in its milder forms. However, in these times of numerous products containing fluoride being available, children ingesting water containing 1 ppm fluoride continue to derive caries protection compared to children ingesting water with negligible amounts of fluoride. Thus, the potential for developing a relatively minor unesthetic condition must be weighed against the potential for reducing dental disease. (Jackson RD,
et al. – J Public Health Dent. 1995 Spring;55(2):79-84)
https://www.ncbi.nlm.nih.gov/pubmed/7484283
Effects of fluoridated
drinking water on bone mass and fractures: the study of osteoporotic fractures:
Our results do not support the findings from recent ecological studies which
showed an increased risk of hip fracture among individuals exposed to fluoridated
public water. (Cauley JA, et al. – J Bone Miner Res. 1995 Jul;10(7):1076-86)
https://www.ncbi.nlm.nih.gov/pubmed/27306248
Fluorides and Oral Health – Report of a WHO Expert Committee on Oral Health Status and Fluoride Use, 1994:
Conclusion of ‘Fluoride in drinking-water’ section: Community water fluoridation is safe and cost-effective and should be introduced and maintained wherever socially acceptable and feasible.
2016 update of Fluoride and Oral Health: Provided that a community has a piped water supply, water fluoridation is the most effective method of reaching the whole population, so that all social classes benefit without the need for active participation on the part of individuals. Water fluoridation has been endorsed by the world’s leading science and health organizations, including WHO, the International Association for Dental Research (IADR) and FDI World Dental Federation.
https://www.ncbi.nlm.nih.gov/pubmed/8259189
Free Article
Acute fluoride poisoning from a public water
system: In May 1992, excess fluoride in one of two public water
systems serving a village in Alaska caused an outbreak of acute fluoride
poisoning. ...We estimated that 296 people were poisoned; 1 person
died. ...The fluoride concentration of a
water sample from the implicated well was 150 mg per liter {150
times normal}, and that of a sample from the other system was 1.1 mg per
liter. Failure to monitor and respond appropriately to elevated fluoride
concentrations, an unreliable control system, and a mechanism that allowed
fluoride concentrate to enter the well led to this outbreak. Discussion:
'The findings of our investigation should be of concern both to health care
providers of patients with acute fluoride poisoning and to public health
and other officials responsible for water fluoridation. The efficacy of
fluoridation in preventing dental caries has been well documented, and the
safety of this practice is supported by the extreme rarity of incidents
of overfluoridation. We believe that the practice of fluoridation of public
water systems should continue. However, public health officials must make
certain that standard safety equipment is installed, that water-system operators
are properly trained, and that routine, systematic monitoring and follow-up
of fluoride concentrations in water systems and inspection of fluoridation
units are undertaken. (Gessner BD, et al. – N Engl J Med. 1994 Jan 13;330(2):95-9)
https://www.ncbi.nlm.nih.gov/pubmed/8500120
Efficacy of preventive
agents for dental caries. Systemic fluorides: water fluoridation: The
effectiveness of fluoridation has been documented by observational and interventional
studies for over 50 years. Data are available from 113 studies in 23 countries.
The modal reduction in DMFT values for primary teeth was 40-49% and 50-59%
for permanent teeth. The pattern of caries now occurring in fluoride and
low-fluoride areas in 15- to 16-year-old children illustrates the impact
of water fluoridation on first and second molars. The secular changes in
caries in Hartlepool, a natural fluoride area in the North East of England,
shows only a modest change between 1949 and 1989. Information on the pre-eruptive
effects of water fluoridation has been reviewed, suggesting that fluoridation
should start at birth to provide optimal protection to primary teeth. At
15 years of age, the maximum DMFS reduction in a fluoridated area was due
about half to the pre-eruptive and about half to the post-eruptive effect
of fluoride. (Murray JJ – Caries Res. 1993;27 Suppl 1:2-8
https://www.ncbi.nlm.nih.gov/pubmed/2066482
Dental caries and
fluoride exposure in Western Australia: Bivariate analysis revealed
all fluoride exposure to be associated with reduced caries experience, but
there were large correlations between some variables. When unconditional
logistic regression analysis was used, the most important (p less than 0.05)
odds ratios associated with no caries experience were for residence in a
fluoridated area from four to 12 years of age and early use of toothpaste.
(Riordan, PJ – J Dent Res. 1991 Jul;70(7):1029-34)
https://www.ncbi.nlm.nih.gov/pubmed/8474047
A half-century of community water fluoridation in the United States: review and commentary:
Abstract - The nearly 50-year history of community water fluoridation is reviewed with the major emphasis on the benefits and safety of fluoridation. Other aspects of water fluoridation also described include the apparent reduction in measurable fluoridation benefits because of the abundance of other fluoride sources, the diffusion of fluoridation effects into fluoride-deficient communities, preeruptive and posteruptive effects, technical and cost aspects, sociopolitical and legal issues that affect the successful fluoridation of communities, and alternatives to community water fluoridation. The majority of studies have evaluated the effectiveness of water fluoridation on the permanent teeth of children, while there are fewer studies on deciduous teeth and in adults; the relationship between fluoride ingestion and bone health needs further clarification; the sociopolitical issues of fluoridation need to be better understood.
(Ripa LW – J Public Health Dent. 1993 Winter;53(1):17-44)
https://www.ncbi.nlm.nih.gov/pubmed/1819282
Caries prevention--fluoride:
reaction paper: Although the prevalence of caries has declined in young
persons in developed countries, there is still a need for water fluoridation.
The effectiveness of fluoride is dependent on the ambient levels of fluoride
in the oral cavity. Fluoride appears to exert the bulk of its protective
effect locally by promoting remineralization of early carious lesions. Nevertheless,
fluoride tablets continue to be prescribed as if the action of fluoride
is expressed systemically. There is an urgent need to explore the clearance
of fluoride from the mouth and to develop methods to ensure constant levels
of fluoride in the oral cavity, thereby reducing both the need for frequent
exposure and the amount necessary for clinical effect. (Bowen WH – Adv Dent
Res. 1991 Dec;5:46-9) {Often, when controversial papers
are published, like the Clarkson paper below, others are offered an opportunity
to respond immediately}
https://www.ncbi.nlm.nih.gov/pubmed/1819281
Caries prevention--fluoride:
Convincing evidence exists that fluoride has a major effect on the demineralization
and remineralization of dental hard tissues, and that it interferes with
the acid production from "cariogenic" bacteria. However, it has
also been shown to be physiologically harmful if fluoride concentrations
and/or exposure periods are inappropriate. ...The benefits and problems
associated with the systemic route of fluoride administration are discussed
with special reference to caries control and fluoride's mechanism of action
and its toxic effect. The same discussions are focused on the role of the
topical effects of fluoride, with particular emphasis placed upon: low vs.
high fluoride concentrations; calcium fluoride vs. fluorhydroxyapatite;
and fluoride distribution, in both the mouth and in the teeth. The benefits
and problems associated with the systemic route of fluoride administration
are discussed with special reference to caries control and fluoride's mechanism
of action and its toxic effect. The same discussions are focused on the
role of the topical effects of fluoride, with particular emphasis placed
upon: low vs. high fluoride concentrations; calcium fluoride vs. fluorhydroxyapatite;
and fluoride distribution, in both the mouth and in the teeth. The benefits
and problems associated with the systemic route of fluoride administration
are discussed with special reference to caries control and fluoride's mechanism
of action and its toxic effect. The same discussions are focused on the
role of the topical effects of fluoride, with particular emphasis placed
upon: low vs. high fluoride concentrations; calcium fluoride vs. fluorhydroxyapatite;
and fluoride distribution, in both the mouth and in the teeth. (Clarkson
BH – Adv Dent Res. 1991 Dec;5:41-5)
https://www.ncbi.nlm.nih.gov/pubmed/2312893
Recent trends in dental caries in U.S. children and the effect of water fluoridation: The decline in dental caries in U.S. schoolchildren, first observed nationwide in 1979-1980, was confirmed further by a second national epidemiological survey completed in 1987. Mean DMFS scores in persons aged 5-17 years had decreased about 36% during the interval, and, in 1987, approximately 50% of children were caries-free in the permanent dentition. Children who had always been exposed to community water fluoridation had mean DMFS scores about 18% lower than those who had never lived in fluoridated communities. When some of the "background" effect of topical fluoride was controlled, this difference increased to 25%. The results suggest that water fluoridation has played a dominant role in the decline in caries and must continue to be a major prevention methodology. (Brunelle JA1, Carlos JP. – J Dent Res. 1990 Feb;69 Spec No:723-7)
https://www.ncbi.nlm.nih.gov/pubmed/12637966
NTP Toxicology and Carcinogenesis Studies of Sodium Fluoride (CAS No.
7681-49-4)in F344/N Rats and B6C3F1 Mice (Drinking Water Studies): There
was no evidence of carcinogenic activity in female F344/N rats receiving
sodium fluoride at concentrations of 25, 100, or 175 ppm (11, 45, or 79
ppm fluoride) in drinking water for 2 years. There was no evidence of carcinogenic
activity of sodium fluoride in male or female mice receiving sodium fluoride
at concentrations of 25, 100, or 175 ppm in drinking water for 2 years.
Dosed rats had lesions typical of fluorosis of the teeth and female rats
receiving drinking water containing 175 ppm sodium fluoride had increased
osteosclerosis of long bones. (Natl Toxicol Program Tech Rep Ser. 1990 Dec;393:1-448)
https://www.ncbi.nlm.nih.gov/pubmed/2129630
Fluoride: Benefits
And Risks of Exposure: Together, these studies indicate that fluoride
in drinking water is beneficial to dental health. However, recent studies
have reported declines in caries prevalence in nonfluoridated areas that
are comparable in magnitude to declines noted in fluoridated areas. While
these estimates of caries decreases in nonfluoridated areas appear accurate,
conclusions cannot be drawn from these studies concerning the independent
effects of fluoridated drinking water on caries prevalence since other possible
sources of fluoride exposure were not measured. Fluoride sources, other
than in drinking water, may provide a level of caries protection similar
to fluoridated drinking water. (Laurence S, et al. – Crit Rev Oral Biol
Med. 1990;1(4):261-81)
https://www.ncbi.nlm.nih.gov/pubmed/2681730
Effectiveness of water fluoridation:
Abstract - The efficacy of communal water fluoridation in reducing dental caries has been reviewed based on surveys conducted in the last decade of caries prevalence in fluoridated and nonfluoridated communities in the United States as well as in Australia, Britain, Canada, Ireland, and New Zealand. The efficacy is greatest for the deciduous dentition, with a range of 30-60 percent less caries in fluoridated communities. In the mixed dentition (ages 8 to 12), the efficacy is more variable, about 20-40 percent less caries. In adolescents (ages 14-17), it is about 15-35 percent less caries. Current data on caries prevalence in adults and seniors are extremely limited and include several populations living in communities with higher than optimal fluoride levels. For these adults and seniors, a range of 15-35 percent less caries would also apply. Viewed in toto, the current data for children, adolescents, adults and seniors show a consistently and substantially lower caries prevalence in fluoridated communities. For an accurate measurement of the efficacy of water fluoridation in reducing dental caries, it is essential that only persons with a record of continuous or long-term residency in fluoridated versus nonfluoridated areas be included in such assessments. Because of the high geographic mobility in our society and the widespread use of fluoride dentifrices, supplements, and other topical fluoride agents, such comparisons are becoming more difficult to conduct. Accordingly, the effectiveness (rather than the efficacy) of water fluoridation has decreased as the benefits of other forms of fluoride have spread to communities lacking optimal water fluoridation.
(Newbrun E – J Public Health Dent. 1989;49(5 Spec No):279-89)
https://www.ncbi.nlm.nih.gov/pubmed/2914978
Treatment of Bone Weakness
in Patients with Femoral Neck Fracture by Fluoride, Calcium, and Vitamin
D: Twenty-three of 46 patients, aged 56 to 95 years, with fracture
of the femoral neck (FNF) completed the first trial of 10 months treatment
with oral sodium fluoride 60 mg and calcium 1800 mg on alternate days and
1 ıtg of vitamin D1 daily. In 17 patients the treatment improved
the amount and quality of trabecular bone. Cortical thickness increased
in nine patients and there were no losses of amount or mineralisation. The
treatment was well tolerated by most patients and there were no major side-effects
or signs of bone demineralisation. The study also revealed an unexpected
rapid post-fracture deterioration of bone tissue in untreated FNF patients;
thus there is an increased risk of further fractures which calls for the
use of an effective treatment to increase bone mass. (Mackie et al. – J
Bone Joint Surg Br 1989 71-B (1): 111)
https://www.ncbi.nlm.nih.gov/pubmed/4025650
Free Article
Fluorides, facts and fanatics: public health
advocacy shouldn't stop at the courthouse door: One of the more controversial
American public health issues is fluoridation of municipal water supplies.
Opponents occasionally succeed in halting fluoridation through local referenda,
but the courts usually uphold fluoridation laws. In 1982, however, an Illinois
trial judge ruled that a state law authorizing fluoridation was unconstitutional.
Although unimpressed by the plaintiff's evidence purporting to show fluoridation's
risks, the judge was compelled to rule against the state because it had
failed to counter with evidence on the safety of fluoridated water. Christoffel
analyzes the trial court's decision and its subsequent reversal by the Illinois
Supreme Court. He urges public health professionals to assume advocacy roles
by ensuring that the scientific rationale behind public health regulations
becomes part of the legislative record and by forcefully supporting public
health policies in all forums, including the courts. (Christoffel T – Am
J Public Health. 1985 Aug;75(8):888-91)
https://www.ncbi.nlm.nih.gov/pubmed/3917599
Free Article
Thirty years of fluoridation: a review: Fluoride
contributes to stability of both teeth and bones and to reduction of caries,
especially if ingested before eruption of teeth. Reduction of caries continues
at about 60% in persons drinking fluoridated water only as long as fluoride
washes over teeth. One-half the population of the US does not have access
to water with an optimal fluoride concentration of about 1 mg/L. Misinformation
about fluoridation contributes to reluctance of communities to supplement
the natural but inadequate fluoride of those water supplies. Fluoridation
of water has no positive or negative effect on incidence or mortality rates
due to cancer, heart disease, intracranial lesions, nephritis, cirrhosis,
mongoloid births, or from all causes together. The collective decision to
increase the natural fluoride content of water supplies is not an infringement
of civil rights, nor does it establish a precedent in the binding sense
of the law. Supplemental fluoride in water makes it available to all members
of the community in a safe, practical, economical and reliable manner. Fluoridation
saves money in dental costs and time lost from work. Fluoridation is an
appropriate action of government in promoting the health and welfare of
society. (Richmond VL – Am J Clin Nutr. 1985 Jan;41(1):129-38)
Fluoridation of Water and Cancer: A Review of the Epidemiological Evidence -
The justification for such a measure as the addition of fluoride to the water supplies of entire communities must rely on strong scientific evidence pointing not only to its effectiveness but to its safety, even though the recommended level in the public water supply is similar to that yielded by many natural sources. From the first, therefore, the safety of the fluoridation of water to the optimum concentration (1 milligram per litre) has been a paramount consideration, and fluoridation programmes were both preceded and accompanied by investigations ofthe health of populations exposed to fluoride in water. Allegations that fluoridation causes cancer have naturally given rise to great public concern.
Authoritative advice on all aspects of the evidence, in relation to the addition of fluoride to the drinking water of whole communities to achieve a concentration of 1 milligram per litre, has recently been obtained from the Department's independent expert scientific advisers. They considered all the available evidence on the biological effects of fluoride in short-term tests, and animal carcinogenicity tests, as well as the direct and extensive studies of human populations reviewed in the present Report.
They concluded that there is no evidence leading to an expectation of hazard through the induction of heritable abnormalities, and no reliable evidence of any hazard to man in respect of cancer.
(1985 Report of the Working Party )
Other download options
https://www.ncbi.nlm.nih.gov/pubmed/6384648
Fluorine and thyroid
gland function: a review of the literature: Published data failed to
support the view that fluoride, in doses recommended for caries prevention,
adversely affects the thyroid. (Bergi H, et al. – Klin Wochenschr. 1984
Jun 15;62(12):564-9)
https://www.ncbi.nlm.nih.gov/pubmed/6360403
Free Article
The alleged association between artificial fluoridation
of water supplies and cancer - a review: Since 1945, artificial fluoridation
of water supplies has been used with success to reduce the incidence of
dental caries in many areas where the natural fluoride content of the water
is low. However, since 1975, it has been maintained that such artificial
fluoridation is followed by an increased risk of cancer. These allegations
originate from a single source. The present review, which covers re-examinations
of the same data as well as evidence from scientific and governmental bodies
in many countries, shows these assertions to be erroneous. (J. Clemmesen
– Bull World Health Organ. 1983; 61(5))
https://www.ncbi.nlm.nih.gov/pubmed/7338695
Free Article
Fluoridation of water supplies and cancer mortality
I: A search for an effect in the UK on risk of death from cancer: Claims
that the mortality from cancer has been increased in urban populations as
a result of the fluoridation of water supplies have been given publicity
in the press and on the radio and television, and questions have consequently
been asked in Parliament with a view to stopping plans for further fluoridation.
These. claims have been based on an analysis of the trend in cancer mortality
rates in American towns by Yiamouyiannis and Burk1" and more recently
on an analysis of crude cancer mortality in two British towns-Birmingham,
where the water supply was fluoridated in October 1964, and Manchester,
where there has been no fluoridation. CONCLUSION: Examination of the trend
in mortality for cancer in the seven cities in England and Wales with populations
of over 400 000* and in England and Wales as a whole between 1959-63 and
1974-8 provides no reason to suppose that any unique factor, such as fluoridation
of the water supplies, has affected the death rate for cancer in Birmingham
since 1964. (Paula Cook-Mozaffari, et al. – Journal of Epidemiology and
Community Health, 1981, 35, 227-232)
https://www.ncbi.nlm.nih.gov/pubmed/7338696
Free Article
Fluoridation of water supplies and cancer mortality
II: Mortality trends after fluoridation: In the past two years
much publicity has been given to Burk's claim that the mortality from cancer
in Birmingham increased sharply following fluoridation of the water supply
in 1964 and, specifically, that it increased more sharply than in other
British towns. This claim is not supported by detailed examination of age-standardised
mortality rates in England and Wales' and we have, therefore, re-examined
the data to see what led Burk to his conclusion. Conclusions Claims that
unusual increases in cancer mortality have occurred in England after fluoridation
have been examined and have been shown to rest on incorrect arithmetic,
on the use of inappropriate statistical methods, and on examination of too
restricted a part of the available data. Studies from other parts of the
world which have examined trends in cancer mortality after fluoridation,
or which have made geographical comparisons between fluoridated and unfluoridated
areas, have been reviewed. There is no evidence either from England and
Wales or from elsewhere in the world that the addition of fluoride to water
supplies has increased the risk of dying from cancer. (Paula Cook-Mozaffari
– Journal of Epidemiology and Community Health, 1981, 35, 233-238)
https://www.ncbi.nlm.nih.gov/pubmed/622448
Free Article
Fluoridation and mortality--an epidemiologic
study of Pennsylvania communities: Fewer health measures have been accorded
more clinical and laboratory research, epidemiologic study, massive clinical
trials of total community populations, and public attention )both favorable
and adverse) than the fluoridation of public water supplies. As a result,
knowledge of the dental and nondental physiological effects of fluoridation
has increased significantly since Grand Rapids, Mich., was first experimentally
fluoridated in 1945. There is now considerable evidence that fluoridation
of community water supplies is both effective and safe. In 1975, the Council
on Foods and Nutrition of the Americal Medical Association updated its earlier
statement confirming the efficacy and safety of fluoridation under controlled
administration. Jackson provides a list of 22 statements and findings supportive
of fluoridation from lay, legal, and professional groups throughout the
world. However, controversy (maintained by a segment of the general public
and professional community) continues regarding possible adverse effects
of fluoridation on human health. The National Cancer Institute and the National
Heart and Lung Institute have recently issued statements that refute
claims suggesting a relationship between fluoridated water and mortality
from cancer and heart disease. No clear evidence was found to suggest that
fluoridation under controlled administration adversely affects overall mortality
or diabetes mortality. Under controlled administration, fluoridation may
have no significant effect on either mortality rate. The inconsistent relationships
found between high levels of fluoride and cerebrovascular disease mortality
require further investigation. (Tokuhata, GK, et al. – Public Health Reports,
Vol. 93, January-February 1978, pp. 60-68)
Free
Article
Statewide Antifluoridation Initiatives: A New Challenge
to Health Workers - Fluoridation of municipal drinking waters remains
an issue of contention in the western United States. Spirited campaigns
recently have been waged in Oregon and Washington by those who oppose fluoridation.
The approach of the opposition was unique: statewide prohibition campaigns
launched simultaneously in neighboring states. The enabling vehicle for
introduction of these campaigns was the public initiative process. ...A
disquieting aspect of these recent campaigns was the central role in each
state of the
National Health Federation. The Federation, based in Monrovia, California,
is "dedicated to the protection of health freedoms," emphasizing
that the patient should be free to choose alternate forms of health care,
and that the choice should be free of governmental restriction or "monopolistic
control". ...The Federation challenges pasteurization of milk,
fluoridation of public water supplies and immunizations, and promotes Laetrile,
Krebiozen, mega-vitamin therapy, naturopathic medicine, chelation therapy,
and a variety of alternative health care practices. (Caswell A, et al. – AJPH January, 1978, Vol. 68, No. 1)
https://www.ncbi.nlm.nih.gov/pubmed/135009
Water fluoridation and congenital malformations: no association -The
incidence of selected congenital malformations in areas with fluoride supplementation
of public water supplies was compared with the incidence in areas where
the water supply is deficient in fluoride. Comparison of the incidences
of several common birth defects (including Down's syndrome) in fluoridated
and nonfluoridated areas revealed no substantial or significant differences
in which there was a consistent pattern for both sets of data. (Erickson
JD – J Am Dent Assoc. 1976 Nov;93(5):981-4)
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC1551218/
Grand Rapids Fluoridation Study—Results Pertaining to the Eleventh Year of Fluoridation:
In all studies the findings show a reduction of 60-65 per cent in the prevalence of caries in the permanent teeth of children born subsequent to the change in water supply. Furthermore, the evidence strongly suggests beneficial effects on teeth which were formed, or erupted, prior to the initiation of water fluoridation.
In all these studies particular attention and interest has been paid to any effects fluoridation might have on other biologic systems of the body. In none of the studies has there been any scientific evidence to suggest an adverse effect on any segment of a rather large population living under divergent environmental conditions. These observations, in conjunction with the fact that millions of people have used naturally fluoridated waters for generations, attest to the complete safety of the procedure.
(Francis A. Arnold, Jr. – Am J Public Health Nations Healthv.47(5); 1957 May)
https://www.ncbi.nlm.nih.gov/pubmed/13007869
Free Article
Urinary fluoride levels associated with use of fluoridated
waters: Surveys in two areas contribute additional evidence that no
hazard of cumulative toxic fluorosis is associated with the use of fluoridated
water containing 100m fluoride. Within 1 week, the concentration of fluoride
in the urine equaled that in the drinking water for adults. For children,
the period of adjustment was considerably longer {3-5 years}. (Zipkin,
RC – Public Health Rep. 1956 August; 71(8))
https://www.ncbi.nlm.nih.gov/pubmed/13007869
Free Article
Toxicological Evidence for the Safety of the
Fluoridation of Public Water Supplies: The extravagance of the variously
motivated statements frequently heard in opposition to fluoridation wherever
it is under consideration may lead officials who must explain this prophylactic
measure to the public to discount the fact that many citizens still remain
unconvinced of the safety of this procedure, despite the assurances of medical,
dental, and public health authorities. CONCLUSIONS: The results of animal
experimentation show that the prolonged intake of quantities of fluoride
too small to induce dental fluorosis does not give rise to any of the nondental
manifestations of chronic intoxication by fluorides. Epidemiologic data
and clinical and radiographic examinations of exposed industrial workers
indicate that only when the fluoride content of a water supply exceeds 5
or 6 ppm will its prolonged usage give rise to detectable osseous changes
and then only in the most susceptible persons. The evidence as a whole is
consistent in offering assurance that bringing the fluoride concentration
in communal water supplies to that known to be optimal for dental health
is a prophylactic public health procedure which has an ample margin of safety.
(Francis F. Heyroth, M.D. – Am J Public Health Nations Health. 1952 December;
42 (12))
Free Article
Studies on Mass Control of Dental Caries Through
Fluoridation of the Public Water Supply: Summary - Fluoridation
of the Grand Rapids public water supply began in January 1945. Analysis
of the 1949 dental examinations at Grand Rapids shows a reduced amount of
dental caries experience when compared with the pre-fluoridation rates of
1944-45. The findings indicate that the reduction is most pronounced in
the younger age groups whose dentition was largely calcified following the
addition of one part per million of fluoride (F) to the previously fluoride-free
public water supply. Sufficient time has not elapsed to evaluate water fluoridation
in the older age groups. (Dean HE, et al. – Public Health Rep. 1950 October
27; 65(43)) [This article starts about 1/2 way through the document - RJ]
Free Article
The Newburgh-Kingston Caries Fluorine Study (Dental
Findings after Three Years of Water Fluoridation): SUMMARY
1) The
DMF rate for permanent teeth shows a consistent downward trend in Newburgh
from 21.0 to 14.8 per 100 permanent teeth. This indicates a saving of 6.5
permanent teeth per 100 in Newburgh as compared with a rate of 21.3 per
100 in Kingston at the last examination. This represents a saving of 30
per cent.
2) Among first molars, which account for the major part of
the caries problem in children, after three years of fluoride experience,
Newburgh's rate was 48.0 DMF per 100 first molars, while Kingston's was
58.7, or a difference of 10.7 DMF per 100 first molars. This represents
a saving of 18 per cent in DMF first molars.
3) The greatest benefits
are noted in the younger age groups.
4) The differences between Newburgh
and Kingston as represented in these data suggest the possibility of benefits
from exposure to fluoridated water subsequent to enamel calcification and
subsequent to eruption of the first molars.
5) We cannot entirely rule
out the possibility of variation in the interpretations of the examiners.
The fact that more than one examiner was used might alter the differences
between Newburgh and Kingston to some extent. However, the size of the differences
in the DMF rates of the two cities is such that it is unlikely that an examiner
bias could vitiate them.
6) These data are preliminary and it will be
necessary to continue collecting data for the proposed duration of the study,
that is, through 1954 to 1956, to obtain additional information concerning
the caries prophylactic value of fluorine. (David B, et al. – Am J
Public Health Nations Health. 1950 June; 40(6))
Return to
Top of References
Studies of three other common water contaminants on health:
Caffeine, Alcohol/Wine, and
Sugar
Compared the potential health risks or benefits of exposure
to caffeine, alcohol and sugar with fluoride. These are just a few of the
papers that you can find during a brief search of PubMed. I searched
for both health risks and health benefits of the different contaminants.
This is not an attempt to start a crusade for or against these contaminants,
rather it's a demonstration to show how nearly any scientific topic can
generate research papers that support nearly any conclusion possible.
Reliable conclusions about complex issues can not be drawn from a quick
overview of the research or by relying on a list of papers that has been
collected to support a specific viewpoint.
In the rather haphazard listing below you can find references to support
claims of harm from the contaminants or references that demonstrate no harm
or even health benefits. One would need to carefully study the context,
design, methods, results and analyses of each paper and have expert knowledge
of the topics to determine which studies were well conducted with valid
conclusions and which were not. Without the understanding to personally
evaluate all of the evidence for a topic one can rely on the believability
and trustworthiness of the expert scientific community to make a decision
on what to believe.
Or, you can rely on the believability
and trustworthiness of small groups that have strong philosophical agendas
that are in opposition to mainstream science and medicine.
In the case of water fluoridation, the mainstream dental, scientific,
and medical communities support drinking water fluoridation precisely because
nearly all subject experts have determined that the evidence of safety and
effectiveness is more substantial, better and outweighs the evidence presented
for harm and ineffectiveness at optimal levles.
Coffee and Caffeine
Health Benefits of Methylxanthines in Cacao and Chocolate: (2013)
The physiological effects of methylxanthines have been known for a long
time and they are mainly mediated by the so-called adenosine receptors.
Caffeine and theobromine are the most abundant methylxanthines in
cacao and their physiological effects are notable. Their health-promoting
benefits are so remarkable that chocolate is explored as a functional food.
Coffee, but not caffeine, has positive effects on cognition and psychomotor
behavior in aging: (2013) The presence of several bioactive
compounds, such as polyphenols and caffeine, implicates coffee as a potential
nutritional therapeutic in aging. Moderate (three to five cups a day) coffee
consumption in humans is associated with a significant decrease in the risk
of developing certain chronic diseases.
Caffeine for treatment of Parkinson disease, A randomized controlled trial:
(2012) Objective: Epidemiologic studies consistently link caffeine,
a nonselective adenosine antagonist, to lower risk of Parkinson disease
(PD). However, the symptomatic effects of caffeine in PD have not been adequately
evaluated. Conclusions: Caffeine provided only equivocal borderline
improvement in excessive somnolence in PD, but improved objective motor
measures. These potential motor benefits suggest that a larger long-term
trial of caffeine is warranted.
Increased caffeine consumption is associated with reduced hepatic fibrosis:
(2010) Conclusion: A reliable tool for measurement of caffeine
consumption demonstrated that caffeine consumption, particularly from regular
coffee, above a threshold of approximately 2 coffee-cup equivalents per
day, was associated with less severe hepatic fibrosis.
Caffeine suppresses β-amyloid levels in plasma and brain of Alzheimer's
transgenic mice: (2009) Recent epidemiologic studies suggest that
caffeine may be protective against Alzheimer's Disease (AD). Our conclusion
is two-fold. First, that both plasma and brain Aβ levels are reduced
by acute or chronic caffeine administration in several AD transgenic lines
and ages, indicating a therapeutic value of caffeine against AD. Second,
that plasma Aβ levels are not an accurate index of brain Aβ levels/deposition
or cognitive performance in aged AD mice.
Caffeine Use in Children: What we know, what we have left to learn, and
why we should worry: (2009) Caffeine is a widely used psychoactive
substance in both adults and children that is legal, easy to obtain, and
socially acceptable to consume. Although once relatively restricted to use
among adults, caffeine-containing drinks are now consumed regularly by children.
In addition, some caffeine-containing beverages are specifically marketed
to children as young as four years of age. Unfortunately, our knowledge
of the effects of caffeine use on behavior and physiology of children remains
understudied and poorly understood.
Maternal
Consumption of Coffee and Caffeine-containing Beverages and Oral Clefts:
(2009) A Population-based Case-Control Study in Norway: Compared
with that for no coffee consumption, the adjusted odds ratios for cleft
lip with or without cleft palate were 1.39 (95% confidence interval: 1.01,
1.92) for less than 3 cups a day and 1.59 (95% confidence interval: 1.05,
2.39) for 3 cups or more.
High
dietary caffeine consumption is associated with a modest increase in headache
prevalence: (2009) In the multivariate analyses, adjusting for age,
gender, smoking, and level of education as confounding factors, a weak but
significant association (OR = 1.16, 95% CI 1.09-1.23) was found between
high caffeine consumption and prevalence of infrequent headache.
The
face of chronic migraine: epidemiology, demographics, and treatment strategies: (2009)
Aside from analgesic overuse, other modifiable risk factors associated with
the development of chronic migraine and CDH must be addressed including
obesity and caffeine use...
Caffeine
Induces Cell Death via Activation of Apoptotic Signal and Inactivation of
Survival Signal in Human Osteoblasts: (2008) Caffeine consumption
is a risk factor for osteoporosis... Here, we show that cell viability decreases
in osteoblasts treated with caffeine in a dose-dependent manner.
Comparing the benefits of Caffeine, Naps and Placebo on Verbal, Motor and
Perceptual Memory: (2008) These findings provide evidence
of the limited benefits of caffeine for memory improvement compared with
napping. We hypothesize that impairment from caffeine may be restricted
to tasks that contain explicit information; whereas strictly implicit learning
is less compromised.
Coffee
and cardiovascular disease risk: yin and yang: (2008)
Many epidemiological
studies have addressed the effects of coffee on cardiovascular disease.
Most case-control studies suggest an increased risk in high coffee consumers,
whereas cohort studies indicate no clear association with cardiovascular
risk... Moreover, coffee contains several biologically active substances
that may have either beneficial or harmful effects on the cardiovascular
system. The development of complete/partial tolerance to some caffeine effects
in habitual drinkers adds to the complexity of coffee effects. Variation
in cup size and methods of coffee preparation may also explain some conflicting
results.
Habitual
coffee consumption and blood pressure: An epidemiological perspective:
(2008) This paper summarizes the current epidemiological evidence on
coffee consumption in relation to blood pressure (BP) and risk of hypertension.
Free Article
Coffee
and caffeine intake and the risk of ovarian cancer: the Iowa Women's Health
Study: (2008) Our results suggest that a component of coffee other
than caffeine, or in combination with caffeine, may be associated with increased
risk of ovarian cancer in postmenopausal women who drink five or more cups
of coffee a day.
Free Article
Potential
teratogenic and neurodevelopmental consequences of coffee and caffeine exposure:
a review on human and animal data: (1994) The teratogenic
effect of caffeine has been clearly demonstrated in rodents. The sensitivity
of different animals species is variable. In humans, caffeine does not present
any teratogenic risk. The increased risk of the most common congenital malformations
entailed by moderate consumption of caffeine is very slight. However, caffeine
potentiates the teratogenic effect of other substances, such as tobacco,
alcohol, and acts synergistically with ergotamine and propranolol to induce
materno-fetal vasoconstrictions leading to malformations induced by ischemia.
Therefore, even though caffeine does not seem to be harmful to the human
fetus when intake is moderate and spread out over the day, some associations,
especially with alcohol, tobacco, and vasoconstrictive or anti-migraine
medications should be avoided. Maternal consumption of caffeine affects
brain composition, especially in case of a low-protein diet and also seems
to interfere with zinc fixation in brain. Maternal exposure to caffeine
induces also long-term consequences on sleep, locomotion, learning abilities,
emotivity, and anxiety in rat offspring, whereas in humans, more studies
are needed to ascertain long-term behavioral effects of caffeine ingestion
by pregnant mothers.
Alcohol & Wine
Wine, Beer, Alcohol and Polyphenols on Cardiovascular Disease and Cancer:
(2012) Since ancient times, people have attributed a variety of health
benefits to moderate consumption of fermented beverages such as wine and
beer, often without any scientific basis. There is evidence that excessive
or binge alcohol consumption is associated with increased morbidity and
mortality, as well as with work related and traffic accidents. On the contrary,
at the moment, several epidemiological studies have suggested that moderate
consumption of alcohol reduces overall mortality, mainly from coronary diseases.
However, there are discrepancies regarding the specific effects of different
types of beverages (wine, beer and spirits) on the cardiovascular system
and cancer, and also whether the possible protective effects of alcoholic
beverages are due to their alcoholic content (ethanol) or to their non-alcoholic
components (mainly polyphenols). Epidemiological and clinical studies have
pointed out that regular and moderate wine consumption (one to two glasses
a day) is associated with decreased incidence of cardiovascular disease
(CVD), hypertension, diabetes, and certain types of cancer, including colon,
basal cell, ovarian, and prostate carcinoma. Moderate beer consumption has
also been associated with these effects, but to a lesser degree, probably
because of beer's lower phenolic content. These health benefits have mainly
been attributed to an increase in antioxidant capacity, changes in lipid
profiles, and the anti-inflammatory effects produced by these alcoholic
beverages.
Moderate Ethanol Ingestion and Cardiovascular Protection: (2011)
While ethanol intake at high levels (3-4 or more drinks), either in acute
(occasional binge drinking) or chronic (daily) settings, increases the risk
for myocardial infarction and ischemic stroke, an inverse relationship between
regular consumption of alcoholic beverages at light to moderate levels (1-2
drinks per day) and cardiovascular risk has been consistently noted in a
large number of epidemiologic studies.
The effects of light to moderate
ethanol consumption appear to be most clearly related to cardiovascular
benefits, with most studies reductions in risk for heart disease by 30-35%.
Regular alcohol consumption at low to moderate levels is associated with
significant reductions in the incidence of myocardial infarction in both
males and females, regardless of age in adults. Importantly, this effect
was noted in higher risk populations, including individuals with diabetes,
hypertension, hypercholesterolemia, known heart disease, or who are overweight,
as well as in cigarette smokers. In addition to reducing the incidence
and severity of myocardial infarction, low to moderate alcohol consumption
is also associated with lower risk for ischemic stroke, dementia, congestive
heart failure, peripheral artery disease, intestinal and hepatic I/R injury,
and frequency of Raynaud's phenomenon. Heart rate variability, a marker
of autonomic imbalance, is also improved by consumption of alcoholic beverages,
with wine intake demonstrating a stronger association with this effect than
beer or spirits. Reductions in C-reactive protein, fibrinogen, interleukin-6,
and tumor necrosis factor alpha also occur with regular moderate alcohol
consumption. The aforementioned observations clearly indicate that the health
benefits of alcohol consumption extend beyond the heart.
Alcohol
in Moderation, Cardioprotection and Neuroprotection: Epidemiological Considerations
and Mechanistic Studies: (2008) In contrast to many years
of important research and clinical attention to the pathological effects
of alcohol (ethanol) abuse, the past several decades have seen the publication
of a number of peer-reviewed studies indicating beneficial effects of light-moderate,
non-binge consumption of varied alcoholic beverages, as well as experimental
demonstrations that moderate alcohol exposure can initiate typically cytoprotective
mechanisms. A considerable body of epidemiology associates moderate alcohol
consumption with significantly reduced risks of coronary heart disease and,
albeit currently a less robust relationship, cerebrovascular (ischemic)
stroke. Experimental studies with experimental rodent models and cultures
(cardiac myocytes, endothelial cells) indicate that moderate alcohol exposure
can promote anti-inflammatory processes involving adenosine receptors, protein
kinase C (PKC), nitric oxide synthase, heat shock proteins, and others which
could underlie cardioprotection. Also, brain functional comparisons between
older moderate alcohol consumers and non-drinkers have received more recent
epidemiological study. In over half of nearly 45 reports since the early
1990's, significantly reduced risks of cognitive loss or dementia in moderate,
non-binge consumers of alcohol (wine, beer, liquor) have been observed,
whereas increased risk has been seen in only a few studies.
Increased systemic and brain cytokine production and neuroinflammation by
endotoxin following ethanol treatment: (2008) Conclusion Acute
increases in serum cytokines induce long lasting increases in brain proinflammatory
cytokines. Ten daily doses of ethanol exposure results in persistent alterations
of cytokines and significantly increases the magnitude and duration of central
and peripheral proinflammatory cytokines and microglial activation. Ethanol
induced differential anti-inflammatory cytokine IL-10 responses in liver
and brain could cause long lasting disruption of cytokine cascades that
could contribute to protection or increased risk of multiple chronic diseases.
First-trimester
maternal alcohol consumption and the risk of infant oral clefts in Norway:
(2008) Compared with nondrinkers, women who reported binge-level drinking
(>or=5 drinks per sitting) were more likely to have an infant with cleft
lip with or without cleft palate (odds ratio = 2.2, 95% confidence interval:
1.1, 4.2) and cleft palate only (odds ratio = 2.6, 95% confidence interval:
1.2, 5.6).
Maternal
periconceptional alcohol consumption and risk for orofacial clefts:
(1999) However, for women who reported weekly or more frequent episodes
of consuming >/=5 drinks per drinking occasion compared with those who
did not, we observed increased risks for isolated (no other major congenital
anomaly) cleft lip with or without cleft palate, odds ratio = 3.4 (95% confidence
interval, 1.1 to 9.7); multiple cleft lip with or without cleft palate,
odds ratio = 4.6 (1. 2 to 18.8); and "known syndrome" clefts,
odds ratio = 6.9 (1.9 to 28. 6).
Carcinogenicity
of acetaldehyde in alcoholic beverages: (2009) In addition to being
produced in ethanol metabolism, acetaldehyde occurs naturally in alcoholic
beverages. Limited epidemiological evidence points to acetaldehyde as an
independent risk factor for cancer during alcohol consumption, in addition
to the effects of ethanol.
Chronic
effects of low to moderate alcohol consumption on structural and functional
properties of the brain: (2009) beneficial or not? The changes
reported in brain shrinkage, grey matter and white matter volume, as a result
of low to moderate alcohol consumption sooner offer support for the contention
that such drinking decreases brain health than for its beneficial effect.
The
role of alcohol in oral carcinogenesis with particular reference to alcohol-containing
mouthwashes: (2008) On the basis of this review, we believe that
there is now sufficient evidence to accept the proposition that alcohol-containing
mouthwashes contribute to the increased risk of development of oral cancer
and further feel that it is inadvisable for oral healthcare professionals
to recommend the long-term use of alcohol-containing mouthwashes.
Sugar, disease and cancer
Glycemic
index, glycemic load and cancer risk: (2013) RESULTS: Dietary
GI was positively associated with the risk of prostate cancer (OR, 1.26
for the highest versus the lowest quartile). A higher dietary GL significantly
increased the risk of colorectal (OR, 1.28), rectal (OR, 1.44) and pancreatic
(OR, 1.41) cancers. No other significant associations were found. CONCLUSIONS:
Our findings suggest that a diet high in GI and GL is associated with increased
risk of selected cancers.
Does high sugar consumption exacerbate cardiometabolic risk factors and
increase the risk of type 2 diabetes and cardiovascular disease? (2012)
In conclusion, data from prospective cohort studies published in the years
2000 - 2011 suggest that sugar-sweetened beverages probably increase the
risk of type 2 diabetes. For related metabolic risk factors, cardiovascular
disease or all-cause mortality and other types of sugars, too few studies
were available to draw conclusions.
Is
sugar consumption detrimental to health? A review of the evidence 1995-2006:
(2010) Many countries set quantitative targets for added sugars,
justifying this by expressing concern about the likely impact of sugar on
weight control, dental health, diet quality, or metabolic syndrome. This
review considers whether current intakes of sugar are harmful to health,
and analyses recent literature using a systematic approach to collate, rank,
and evaluate published studies from 1995-2006. Results from high quality
obesity studies did not suggest a positive association between body mass
index and sugar intake. Some studies, specifically on sweetened beverages,
highlighted a potential concern in relation to obesity risk, although these
were limited by important methodological issues. Diet adequacy appeared
to be achieved across sugar intakes of 6 to 20% energy, depending on subject
age. Studies on metabolic syndrome reported no adverse effects of sugar
in the long-term, even at intakes of 40-50% energy. The evidence for colorectal
cancer suggested an association with sugar, but this appeared to have been
confounded by energy intake and glycemic load. There was no credible evidence
linking sugar with attention-deficit, dementia, or depression. Regarding
dental caries, combinations of sugar amount/frequency, fluoride exposure,
and food adhesiveness were more reliable predictors of caries risk than
the amount of sugar alone. Overall, the available evidence did not support
a single quantitative sugar guideline covering all health issues.
Soft drink and juice consumption and risk of pancreatic cancer: the Singapore
Chinese Health Study: (2010) CONCLUSION: Regular consumption
of soft drinks may play an independent role in the development of pancreatic
cancer.
Dietary
habits and risk of pancreatic cancer: an Italian case-control study:
(2009) CONCLUSIONS: The present study supports an inverse association
between fruits and vegetables and pancreatic cancer risk, and it confirms
a direct relation with meat. The increased risk for table sugar suggests
that insulin resistance may play a role in pancreatic carcinogenesis.
Glycemic index, carbohydrates, glycemic load, and the risk of pancreatic
cancer in a prospective cohort study: (2009) Participants
with high free fructose and glucose intake were at a greater risk of developing
pancreatic cancer. Our results do not support an association between glycemic
index, total or available carbohydrate intake, and glycemic load and pancreatic
cancer risk. The higher risk associated with high free fructose intake needs
further confirmation and elucidation.
Sweets, sweetened beverages, and risk of pancreatic cancer in a large population-based
case-control study: (2009) CONCLUSION: These results provide limited
support for the hypothesis that sweets or sugars increase pancreatic cancer
risk.
Added
sugar and sugar-sweetened foods and beverages and the risk of pancreatic
cancer in the National Institutes of Health-AARP Diet and Health Study:
(2008) CONCLUSION: Our results do not support the hypothesis
that consumption of added sugar or of sugar-sweetened foods and beverages
is associated with overall risk of pancreatic cancer.
Glycemic index, glycemic load, and risk of digestive tract neoplasms: a
systematic review and meta-analysis: (2009)
BACKGROUND:
Habitual consumption of diets with a high glycemic index (GI) and a high
glycemic load (GL) may influence cancer risk via hyperinsulinemia and the
insulin-like growth factor axis. CONCLUSIONS: The findings from our meta-analyses
indicate that GI and GL intakes are not associated with risk of colorectal
or pancreatic cancers. There were insufficient data available regarding
other digestive tract cancers to make any conclusions about GI or GL intake
and risk.
Glycemic index, glycemic load, and cancer risk: a meta-analysis: (2008)
CONCLUSION: This comprehensive meta-analysis of Glycemic Index and Glycemic
Load and cancer risk suggested an overall direct association with colorectal
and endometrial cancer.
Glycemic
index, glycemic load, and chronic disease risk--a meta-analysis of observational
studies: (2008) CONCLUSIONS: Low-GI and/or low-GL diets are
independently associated with a reduced risk of certain chronic diseases
(type 2 diabetes, coronary heart disease. In diabetes and heart disease,
gallbladder disease & breast cancer), the protection is comparable with
that seen for whole grain and high fiber intakes. The findings support the
hypothesis that higher postprandial glycemia is a universal mechanism for
disease progression.
Pancreatic
cancer: a review of the evidence on causation: (2008) Pancreatic
cancer kills more than 250,000 people each year worldwide and has a poor
prognosis. The aim of this article is to critically review the epidemiologic
evidence for exposures that may either increase or decrease the risk. A
Medline search was performed for epidemiologic studies and reviews published
up to April 2007. Consistent evidence of a positive association was found
for family history and cigarette smoking. Many studies documented a positive
association with diabetes mellitus and chronic pancreatitis, although the
etiologic mechanisms are unclear. Other associations were detected, but
the results were either inconsistent or from few studies. These included
positive associations with red meat, sugar, fat, body mass index, gallstones,
and Helicobacter pylori, and protective effects of increasing parity, dietary
folate, aspirin, and statins. There was no evidence linking alcohol or coffee
consumption with an increased risk of pancreatic cancer. The associations
with many exposures need to be clarified from further epidemiologic work
in which there is both precise measurement of risk factors, adjustment for
potential confounders, and, for dietary studies, information recorded on
the method of food preparation and pattern of consumption. Such work is
important to reduce the incidence of this fatal disease.
Glycemic load, glycemic index, and pancreatic cancer risk in the Netherlands
Cohort Study: (2008) CONCLUSIONS: Overall, our findings do
not support the hypothesis that GL, GI, or intake of carbohydrates and mono-
and disaccharides are positively associated with pancreatic cancer risk.
This is in agreement with previous prospective studies that investigated
the relation between GL and GI and pancreatic cancer risk.
Added sugar and sugar-sweetened foods and beverages and the risk of pancreatic
cancer in the National Institutes of Health-AARP Diet and Health Study:
(2008) BACKGROUND: Although it has been hypothesized that hyperglycemia,
hyperinsulinemia, and insulin resistance are involved in the development
of pancreatic cancer, results from epidemiologic studies of added sugar
intake are inconclusive. CONCLUSION: Our results do not support the hypothesis
that consumption of added sugar or of sugar-sweetened foods and beverages
is associated with overall risk of pancreatic cancer.
Dietary glycemic load, added sugars, and carbohydrates as risk factors for
pancreatic cancer: the Multiethnic Cohort Study: (2007) Discussion:
In the Multiethnic Cohort Study, high sugar intake-specifically, fructose
intake was associated with a greater risk of pancreatic cancer. This association
was not reflected in the consumption of sodas, but we did observe a greater
risk with a higher intake of fruit and juices. Statistical evidence for
an interaction of sucrose intake with BMI was present, and it showed a higher
risk of pancreatic cancer in overweight or obese study participants with
higher sucrose consumption. To date, 4 prospective studies have investigated
dietary GL and various carbohydrates in relation to pancreatic cancer risk.
Two of these studies found no association for GL, GI, total carbohydrates,
total sugar, sucrose, or fructose, and one study found a greater risk with
higher dietary GL, GI, and fructose intake in sedentary women with a BMI
25, but not in the overall cohort. In the present study, fructose intake
was associated with the highest risk of pancreatic cancer. A subsequent
analysis of high consumption of soft drinks in this same study population
showed significantly greater risks in women but not in men. The present
study also found a positive association between fructose intake and pancreatic
cancer risk, but we did not see a greater risk with higher intake of sodas;
these results did not differ significantly between men and women. ...The
finding of a greater risk with higher fruit and juices intake was surprising,
and it merits some discussion. Fruit, most often in combination with vegetables,
generally is thought to have beneficial effects in terms of cancer prevention
at various sites, including the pancreas. To date, 7 prospective studies
have reported on fruit intake and pancreatic cancer risk, and none detected
a significant association, either positive or inverse. A recent study from
Sweden included 135 pancreatic cancer cases in a cohort of 81 922 men and
women . When the highest and lowest quartiles were compared, overall fruit
intake was not significantly associated with pancreatic cancer risk, nor
was citrus fruit intake. CONCLUSIONS: High fructose and sucrose intakes
may play a role in pancreatic cancer etiology. Conditions such as overweight
or obesity in which a degree of insulin resistance may be present may also
be important.
Glycemic
load, glycemic index, and carbohydrate intake in relation to pancreatic
cancer risk in a large US cohort: (2007) CONCLUSION: Overall,
our data do not support the hypothesis that glycemic load or index, or carbohydrate
intake are associated with a substantial increase in pancreatic cancer risk;
however, a weak positive association cannot be ruled out.
Consumption of sugar and sugar-sweetened foods and the risk of pancreatic
cancer in a prospective study: (2006) CONCLUSION: High consumption
of sugar and high-sugar foods may be associated with a greater risk of pancreatic
cancer.
Sugar-sweetened soft drink consumption and risk of pancreatic cancer in
two prospective cohorts: (2005) CONCLUSION: Although soft
drink consumption did not influence pancreatic cancer risk among men, consumption
of sugar-sweetened soft drinks may be associated with a modest but significant
increase in risk among women who have an underlying degree of insulin resistance.
Glycemic
index, glycemic load, and pancreatic cancer risk: (2005) Our
data suggest that overall lycemic index and glycemic load, as well as total
sugar and total carbohydrate intake, are not associated with pancreatic
cancer risk. However, given the limited literature regarding the role of
diet in the etiology of pancreatic cancer, particularly with respect to
glycemic index/load, further investigation is warranted.
Epidemiology
of pancreatic cancer: (2004) A known cause of pancreatic cancer
is tobacco smoking. This risk factor is likely to explain some of the international
variations and gender differences. A number of studies observed a reduction
in pancreatic cancer risk within a decade after smoking cessation, when
compared to current smokers. With tobacco smoking as an exception, risk
factors for pancreatic cancer are not well-established. ...Chronic pancreatitis
and diabetes mellitus are medical conditions that have been consistently
related to pancreatic cancer. Data from numerous studies suggest that these
conditions are likely to be causally related to pancreatic cancer, rather
than being consequences of the cancer. Recent cohort studies, which are
less prone to biases than case-control studies, suggest that obesity increases
the risk of pancreatic cancer. Other studies support the hypothesis that
glucose intolerance and hyperinsulinemia are important in the development
of pancreatic cancer. Other potential risk factors include physical inactivity,
aspirin use, occupational exposure to certain pesticides, and dietary factors
such as carbohydrate or sugar intake.
Dietary sugar, glycemic load, and pancreatic cancer risk in a prospective
study: (2002) CONCLUSION: Our data support other findings
that impaired glucose metabolism may play a role in pancreatic cancer etiology.
A diet high in glycemic load may increase the risk of pancreatic cancer
in women who already have an underlying degree of insulin resistance

 Harvard
Study Finds Fluoride Lowers IQ - Published in Federal Gov't Journal
- This 2012 REUTERS press release (since vanished from the archives)
is a very effective way to grab your attention, and even though
the headline is a false representation of the study's actual stated
conclusions, slightly different versions are still used by fluoridation
opponents. Fear is an extremely powerful motivator.
If you are scared about your safety or the safety of your family
and friends, you are likely to take the most obvious protective
action quickly without wasting time studying the nuances of your
possible options. The same "news story" was published by
other pay-for-distribution platforms like
Harvard
Study Finds Fluoride Lowers IQ - Published in Federal Gov't Journal
- This 2012 REUTERS press release (since vanished from the archives)
is a very effective way to grab your attention, and even though
the headline is a false representation of the study's actual stated
conclusions, slightly different versions are still used by fluoridation
opponents. Fear is an extremely powerful motivator.
If you are scared about your safety or the safety of your family
and friends, you are likely to take the most obvious protective
action quickly without wasting time studying the nuances of your
possible options. The same "news story" was published by
other pay-for-distribution platforms like

 Harvard
Study Finds Fluoride Lowers IQ - Published in Federal Gov't Journal
Harvard
Study Finds Fluoride Lowers IQ - Published in Federal Gov't Journal And
that brings us back to fear! If you truly and passionately believe
the fluoride ion is a deadly poison that is certain to cause great harm
to anyone who is exposed to small amounts (or even if you have a quiet little
voice nattering away in your mind, "Gee, these are pretty
scary claims."), think about how you react to new frightening 'evidence'.
It will likely be easy to continue accepting fervently presented evidence
alleged to show great harm to almost all aspects of human health from fluoridation
opponents. It will probably be quite difficult to consider accepting
evidence that demonstrates benefits of better dental health that appears
to be associated with very small risks of harm from fluoridation supporters.
And
that brings us back to fear! If you truly and passionately believe
the fluoride ion is a deadly poison that is certain to cause great harm
to anyone who is exposed to small amounts (or even if you have a quiet little
voice nattering away in your mind, "Gee, these are pretty
scary claims."), think about how you react to new frightening 'evidence'.
It will likely be easy to continue accepting fervently presented evidence
alleged to show great harm to almost all aspects of human health from fluoridation
opponents. It will probably be quite difficult to consider accepting
evidence that demonstrates benefits of better dental health that appears
to be associated with very small risks of harm from fluoridation supporters.
 Continue
to question the reasons why most of the professionals in a wide variety
of disciplines related to the sciences medicine and dentistry, have
not joined the anti-fluoridation movement if the evidence against
fluoridation is really as damning, as obvious, and as compelling as
portrayed.
Continue
to question the reasons why most of the professionals in a wide variety
of disciplines related to the sciences medicine and dentistry, have
not joined the anti-fluoridation movement if the evidence against
fluoridation is really as damning, as obvious, and as compelling as
portrayed. Carefully
examine the affidavit an anti-fluoridation site challenges dentists to sign.
This is one of the better examples to illustrate how some fluoridation opponents
apparently don't understand how science works.
Carefully
examine the affidavit an anti-fluoridation site challenges dentists to sign.
This is one of the better examples to illustrate how some fluoridation opponents
apparently don't understand how science works.