Summary:
Support Community Water Fluoridation
Introduction:
Primary Fact:
There are two completely contradictory and mutually exclusive interpretations
and presentation of the evidence regarding the safety and effectiveness of
community water fluoridation (CWF) based on exactly the same scientific evidence
which is available to those on both sides of the argument.
Critical Questions:
How can someone who is not a fully trained and experienced scientist &/or health
professional specializing in fluoridation-related health issues (particularly
those who are responsible for making decisions that impact the health and safety
of members of their community) evaluate the accuracy and relevance of complex
scientific evidence?
How can someone who is not a fully trained and experienced scientist &/or health
professional determine who they should accept as a trustworthy expert to
present a fair, accurate evaluation of the evidence – Pro-CWF or Anti-CWF
representatives?
Critical Facts and Questions:
1.
2.
3.
Major, respected science and health organizations do not
post warnings about any health risks of CWF.
(link)
4.
No major, respected science or health organizations
in the world support the anti-fluoridation opinions that CWF is ineffective &/or
harmful to health as legitimate.
There is also absolutely no evidence that a significant number of science &/or
health professionals oppose CWF.
Carefully examine the ideology of organizations that oppose CWF and the credentials and history of those who vigorously oppose the practice.
(link)
5.
·
Q2 –
Why do only a relatively small number of trained and experienced scientists &/or
medical professionals support the anti-fluoridation agenda and beliefs?
6.
Since there are only a relatively few scientists and health professionals,
virtually no mainstream scientific organizations, a few alternate health groups
and some questionable supporters of the anti-fluoridation arguments that CWF is
dangerous and ineffective –– and it can be easily demonstrated that the
available ant-fluoridation ‘evidence’ is presented inaccurately –– how is it
possible that FOs are often successful in their efforts to ban or stop community
water fluoridation? (link)
7.
The
anti-science tactics
employed by FOs
(and others who dismiss an established scientific consensus) to try and convince
members of the public to trust their proclamations that CWF is dangerous,
unethical and ineffective over the conclusions of mainstream science and health
professionals must be exposed so they can be understood and dismissed by
rational, caring members of the public.
(link)
Specifically, FOs:
(a.)
Ignore the scientific consensus; (b.)
Hijack the democratic process; (c.)
Employ fear mongering; (d.) Employ
Gish Gallop tactics; (e.) claim accidents with some link to
fluorine happen, so CWF should be banned; (f.)
Create a veneer of science; (g.)
Blur Ethics and Science; (h.)
Misrepresent Freedom of Choice; (i.) Provide misleading claims
about other countries and CWF; ( j.) Make public, libelous
claims against science and health professionals who support CWF; (k.)
Make false, out-of-context, irrelevant, misleading presentations of
article/study conclusions.
8.
Bottom Line:
I appreciate your
willingness to examine arguments for trusting the overwhelming majority of
scientists and health professionals and the scientific consensus over the
outlier, anti-fluoridation opinions. There are dozens of factors that can increase or decrease the risk of dental
decay. All methods known to increase risk should be minimized and all methods
that reduce the risk (including fluoridation) should be implemented.
Legitimate Science vs. Anti-Science – Additional Fluoridation References:
Two interesting articles about public response to fluoridation in the
1950s - Anti-fluoridation arguments have changed little in over over 65 years.
Should We Put Fluorides In Our Water - MACLEANS, 1953.pdf
Fight Over Fluoridation - Saturday Evening Post, 1956.pdf (images)
Support Community Water Fluoridation –
Trust the Experts Instead of Accepting the
Arguments of Fluoridation Opponents
(Full Discussion)
Introdction: I wish it were as easy to counter anti-fluoridation arguments as simply stating that virtually all claims made by fluoridation opponents (FOs) were flawed and erroneous (which they are). Unfortunately, those anti-F arguments are often presented using effective strategies that make them appear believable to many voters and elected officials. To effectively counter very simple anti-fluoridation arguments like “Fluoride is a poison that should never be put in drinking water” requires paragraphs of detailed explanations and supporting evidence to even uhave a chance at refuting the claim. My detailed explanation, complete with specific supporting evidence, is over 30 pages long with many links to supporting evidence. If you are considering the possibility that anti-fluoridation arguments might have some validity, I hope you will choose to read this presentation of reasons to reconsider your position. If you would prefer to read a shorter outline before tackling the entire set of arguments and evidence, this summary is much shorter but contains fewer details and less supporting evidence.
Community water fluoridation (CWF) has been an important public health measure since the early
1950s after it was first tested successfully in
Grand Rapids, Michigan in 1945.
That initial test was the result of nearly
20 years of scientific investigation
which provided evidence that exposure to fluoride ions (F–) in
drinking water at about 1 ppm appeared to significantly reduce the risk of tooth
decay – while limiting the risk of dental fluorosis.
Since that discovery and the effectiveness of the Grand Rapids
experiment, a number of countries have implemented CWF programs.
Based on the success of CWF, other F– based dental health
measures have been developed and successfully employed like fluoridated
toothpaste, fluoride rinses and varnishes and, in some countries, fluoridated
salt and milk.
However, there has been opposition to CWF since the beginning, and decisions on
whether to fluoridate drinking water (or not) have usually been made in the U.S.
and other countries by a majority of voters or government officials elected by
the voters, not by a majority of science or health experts.
An important dilemma is that most of those voters and elected officials
are not trained scientists &/or health professionals.
Consequently, the decisions of most voters and elected policy-makers
concerning CWF are not (and cannot be) based on their personal evaluation of the
relevant body of complex scientific evidence.
My contention in the following discussion is that the democratic process (if it
is to produce legitimate science-based results beneficial to the population it
is supposed to protect) requires an accurate, impartial consideration of topics
by fair-minded, well-informed voters and elected officials.
The question I attempt to address in the discussion is:
If political decisions that impact
public health issues based on complex scientific evidence are made by the
majority of voters and elected officials who don’t have the training and
experience necessary to personally evaluate the evidence, how can these
individuals determine what the best decisions are regarding CWF – particularly
when they encounter diametrically opposed, mutually exclusive arguments for and
against CWF? The same question
and concerns are relevant to vaccination policies, climate-related decisions,
education policies regarding young-earth creationism, implementing & following
pandemic safety measures (wearing masks, social distancing, appropriate
isolation, etc.), and other science-based issues that impact public policies and
public health measures.
I am a scientist, and I have studied fluoridation issues for over 25 years.
I believe that anti-fluoridation arguments, tactics and the consequences
to public health are dangerous, as are anti-vaccination arguments, ignoring
science-based methods to limit the spread of a pandemic and the rejection of
other science-based policies.
I have actively and publicly engaged in countering
anti-F– arguments since 2015
when FOs launched a serious effort to stop fluoridation of Denver Water.
Fortunately, the Denver Water Board members carefully researched the
issue, trusted the overwhelming majority of experts and the scientific
consensus, and they voted to continue fluoridation.
Even after hearing a presentation by Paul Connett, one of the top
anti-fluoridation activists, the Board concluded “Nothing
has been presented to the Board or learned in our research that would justify
ignoring the advice of these public health agencies and medical and community
organizations, or deviating from the thoroughly researched and documented
recommendation of the U.S. Public Health Service.”
https://www.denverwater.org/sites/default/files/fluoride-board-resolution-august-2015.pdf
12 years earlier, the Fort Collins, CO City Council had to make a similar
decision. A ‘fluoride technical
study group’ responsible for reviewing all evidence for/against CWF was created,
The study group was presented with arguments from fluoridation opponents, yet
the findings on CWF effectiveness, health risks, costs and other risks were all
in favor of CWF – resulting in one of the more detailed CWF evaluations
available.
https://www.fcgov.com/utilities/img/site_specific/uploads/fluoride-report030903.pdf
I am fully aware that there has been
recent research
since the Fort Collins decision and Denver fluoridation battle which FOs have
presented to the public, allegedly as sufficient proof that CWF can reduce IQ
and cause ADHD and other neurological problems – not to mention ongoing claims
CWF causes arthritis, bone fracture, cancer, cardiovascular disease, diabetes,
GI effects, hypersensitivity, kidney disease, male fertility and pineal gland
issues, skeletal fluorosis and thyroid disease. (fluoridealert.org/issues/health/)
Anyone who is responsible for making decisions about
CWF will probably have been sent hundreds of letters from FOs that provide reams
of “conclusive evidence” that allegedly proves CWF is responsible for all the
damaging health issues listed above in addition to claims that CWF amounts to
the illegal addition of medication to the water supply that forces everyone to
drink a poison.
Anyone who is responsible for making decisions about
CWF will also have received letters from scientists and health professionals who
claim that, despite the strongly held opinions and claims of FOs, the overall
body of scientific evidence has continued to support the safety and
effectiveness of fluoridation since 1945 when fluoridation was first tested.
Anyone who has encountered anti-fluoridation claims
will understand that a significant proportion of the arguments consist of
presenting evidence based on published studies that allegedly prove the claims
that CWF is ineffective and actually causes serious damage to the health of
those who drink it. However, to
personally understand and evaluate the validity of evidence provided by FOs
requires significant science or health-care training and experience.
As noted earlier, most members of the public who are elected community
decision makers and/or voters responsible for making choices on CWF and other
science-based public health measures (like vaccination and how to cope during a
pandemic) are not trained scientists or health care professionals.
My goal is to provide accurate facts, a description of anti-F– tactics and convincing evidence in favor of accepting the conclusions of most relevant science and health experts (and the organizations that represent them) that CWF is a safe, effective, ethical science-based public health measure (like drinking water disinfection, vaccination programs and science-based methods for handling a pandemic) for reducing the risk of dental decay and protecting the health of citizens –– without having to present a detailed evaluation of the specific scientific evidence that has led to those science-based conclusions. If you believe that most scientists and health care professionals responsible for public health care practices actually care about others, have relevant training and experience and try their best to make and promote effective, science-based decisions that will benefit their fellow citizens, I encourage you to read the following information.
An important fact:
There are two completely contradictory and mutually exclusive
interpretations and presentation of the evidence regarding the safety and
effectiveness of CWF:
1.
Pro-CWF:
An important and ethical public health measure that significantly lowers
risk of tooth decay and related health problems with no proven health risks that
cause concerns.
2.
Anti-CWF:
An unethical method of forced medication that does not significantly
reduce tooth decay
rates and significantly contributes to an increased risk of lower IQ, ADHD,
cancer, thyroid problems, etc. – as referenced earlier.
·
The Pro-CWF and Anti-CWF conclusions are based on
exactly the same scientific evidence
which is available to those on both sides of the argument.
That creates a serious dilemma for non-scientists.
Some thoughts regarding the evidence provided regarding science-based decisions:
I.
The supporting evidence is generated, selected,
interpreted and presented to the public quite differently by representatives of
the different sides.
II.
The body of scientific evidence relevant to CWF is
extremely complex and extensive – there are many hundreds of studies of varying
quality, disparate relevance and sometimes conflicting conclusions that cover
over
seven decades of research.
III.
Since there is no secret cache of evidence available
to one side of the argument or the other, the real issue is how that body of
scientific evidence is evaluated and how conclusions are reached and presented
to the relevant science and health communities to influence the scientific
consensus.
Perhaps even more important is how
the conclusions are presented to those members of the public (who are not
trained and experienced scientists or health professionals) to influence health
policy decisions. Are studies
conducted, evidence evaluated and conclusions presented fairly and accurately,
or is the goal to accumulate and present ‘evidence’ that supports a
strongly-held belief that must be protected.
IV.
Who decides which selections and interpretations of
the evidence are valid, science-based and legitimate, and how is that
information presented to the public?
V.
As discussed below (Fact 2.), the major science and
health organizations in the world do not accept the conclusions of the
FOs (or, for that matter, vaccination opponents).
If the FOs’ or vaccination opponents’ interpretation of the evidence is
true, and the mainstream science and health organizations that support CWF and
vaccination are completely wrong, how can
the mainstream organizations be trusted to provide accurate information for any
other science-based health issues?
VI.
As described below, most scientists and health
professionals are Pro-CWF, but some FOs do have science/health degrees and
experience.
A Critical Question:
How can someone who is not a fully
trained and experienced scientist &/or health professional specializing in
fluoridation-related health issues (particularly those who are responsible for
making decisions that impact the health and safety of members of their
community) evaluate the accuracy and relevance of complex scientific evidence?
How can they determine which of the completely contradictory pro-CWF and
anti-CFW claims are legitimate and should be followed for the benefit of their
constituents &/or fellow citizens?
My
answer: Most people can’t – they must, at some level, depend on the evaluation and
conclusions of someone they accept as a trustworthy expert; and that would
either be a CWF supporter or opponent.
That
leads to another important question to consider: How can someone who
is not a fully trained and experienced scientist &/or health professional
determine who they should trust to present an accurate evaluation of the
evidence – Pro-CWF or Anti-CWF representatives?
Do they toss a coin? Do they
immediately trust an expert whose conclusions align with their beliefs?
Or do they try to be as diligent and impartial as possible and carefully
consider not only the conclusions presented, but who is presenting the
conclusions, how the evidence is presented and the tactics used to present and
support the conclusions.
This decision of who to trust for guidance on
important, science-based issues is critical, not only for CWF and other health
related issues like vaccination, other water treatment processes and how to deal
with a pandemic, but all other science-based issues and controversies like
evolutionary theory, GMO crops, fears of electromagnetic radiation, etc.
Hopefully a considered evaluation
of important facts that apply to the proponents of both sides of the conflicting
views will be undertaken before a decision is made about who should be
considered a trusted scientific expert on CWF and on all other important
science-based issues.
More information here
Below are some important facts and questions to
encourage your trust and acceptance of Pro-CWF representatives of the
well-established, 75-year scientific consensus that CWF is a safe and effective
public health measure –– regardless of political persuasion and without
resorting (initially anyway) to a detailed evaluation of the evidence –– over
the Anti-CWF claims by that fluoridation is harmful and ineffective:
1.
Fact – It is Important to Understand How Science-Based Conclusions
are Made
–
and how they differ from conclusions based on
NotScience
beliefs
(morals, religion, philosophy, laws, arts and politics): Scientific
understanding of the natural world is constantly evolving.
The continual possibility of change in any scientific consensus based on
legitimate scientific research is one of the most unique, important and often
misunderstood characteristics of science. (My detailed explanation of
What Is
Science)
However, without a reliable process that allows for a change in consensus based
on a fair and accurate evaluation of evolving evidence, science would either be
an unchanging, authoritarian belief system, and all of the characteristics of
modern society which are based on an evolving understanding of the natural world
would not exist –– or scientific understanding resemble a pinball game.
continually changing and bouncing around from new idea - to new idea - to new
idea, and nothing would be accomplished.
It is critical to understand the difference between:
a.
scientists who
dispute an established scientific consensus and use legitimate, relevant,
accurately presented, reproducible scientific evidence to convince relevant
experts the consensus needs changing, and
b.
those who
don’t have the evidence to change the scientific consensus, abandon the
scientific communities and try to change public opinion instead.
**
Science, in any area of study –
including fluoridation – can only progress by serious challenges to an accepted
scientific consensus by legitimate scientists who acquire and present newly
acquired legitimate evidence and who work within the scientific communities to
convince other legitimate scientists their evidence is good quality, is fairly
represented, is reproducible by others (who will probably be skeptical), and is
actually a fair and legitimate challenge to the current consensus.
When those criteria are met the consensus can begin to change – and
scientific knowledge (which impacts all of society) progresses.
a.
Mother Nature
does not care one whit about politics or any strongly-held personal beliefs.
If you jump off a cliff without taking proper science-based precautions,
it does not matter how strongly-held your dismissal of gravity and belief in
personal levitation might be, you will pay the natural consequences.
b.
Virtually any
scientific issue is complex – even for scientists.
There may be thousands of studies conducted over many decades on any
given sub-specialty – like fluoridation, vaccination, evolution, climate issues
– and the quality and reliability of those studies will range from excellent to
poor. Some studies will be
reproducible and some won’t. Some
studies will be designed, conducted and evaluated reasonably and impartially –
some will be designed, conducted and evaluated with strong desires for a
pre-defined outcome and conclusions.
c.
For any given
science-based issue, the available body of evidence is evaluated by relevant
experts who determine the quality, relevance and reproducibility of each study,
and they formulate the best conclusion possible from all the evidence (a scientific consensus).
Obviously, this is a complex process and there is often disagreement
among the experts. Therefore the
consensus represents a majority viewpoint at any given time, and it is subject
to constant review and modification as new legitimate, reproducible evidence is
produced. Despite potential
complications and disputes, a scientific consensus is the best explanation of
the data at any given time and is adopted by the majority of relevant experts.
(Wikipedia,
Rationalwiki,
Bloomberg).
d.
In order to
change the scientific consensus, legitimate, compelling, reproducible scientific
evidence must be presented. For over 70 years, FOs have been completely unable
to provide a single high-quality, convincing, legitimate, reproducible,
scientific study to support their claims that drinking optimally fluoridated
water is ineffective or harmful to health. The scientific consensus that
fluoridation is safe and effective has not changed.
Those who dismiss acceptance of
the scientific consensus as the most reliable conclusion to trust regarding
complex scientific issues, have never provided a workable alternative
– except to just ignore the consensus and blindly adopt their conclusions.
e.
Consequently,
there is a critical difference between legitimate scientists and health care
providers who challenge an accepted scientific consensus and follow the
established protocols of working within the scientific community to effect
change, and anti-science activists who demand change based only on their strong,
inflexible, unsupported beliefs – examples include anti-vaccination activists,
anti-fluoridation activists, young-earth/Noah’s-flood activists,
anti-water-disinfection activists, activists who believe there is no
relationship between climate change and human activities, and the new wave of
hydroxychloroquine-‘cure’/anti-mask/anti-distancing
fanatics.
f.
As described above, legitimate scientists &/or health care
providers do not morph into anti-science activists just because they disagree
with a scientific consensus.
Scientists or health care providers morph into Anti-Science Activists when:
o
The
morphing anti-science activists (MA-SAs)
have extremely strong, inflexible philosophical, political, ethical &/or
spiritual beliefs (or business goals) which conflict with a specific scientific
consensus.
o
The evidence
MA-SAs claim to have in support of their beliefs is not of convincing quality,
has been misrepresented &/or is not reproducible.
Consequently, they are unable to convince relevant expert scientists to
consider changing the consensus.
o
MA-SAs then
choose to abandon working within the scientific community to produce more
substantial, high-quality supporting evidence.
o
The MA-SAs
choose not to work with other scientists to better explain their evidence and
perhaps convince the scientific community their evidence and interpretations are
valid.
o
MA-SAs choose
not to assist others to successfully reproduce and confirm their experimental or
observational results.
o
MA-SAs then
choose to take their beliefs and their interpretation of the evidence directly
to the public in a deliberate effort to bypass the processes of science and
hijack the democratic process.
o
MA-SAs adjust
and present their ‘evidence’ in a manner (often employing disingenuous, false
fear-mongering tactics) that is most likely to sway public opinion and cause
well-meaning individuals who don't have relevant scientific training or
experience to join their cause.
o
MA-SAs don't
correct members of the public who further distort the available ‘evidence’ as
they originally presented it – or those who even completely fabricate claims.
o
MA-SAs argue
to the public that their interpretation of their ‘evidence’ is more legitimate
than the interpretation of the vast majority of evidence by the overwhelming
majority of scientists they disagree with.
o
MA-SAs often
promote the idea that mainstream scientists and health care professionals who
support the scientific consensus should not be trusted because they are part of
some vaguely defined (and completely unproven) conspiracy – or they have not
bothered to adequately understand and evaluate the evidence and just blindly
accept the position of others.
o
At that point
the scientists &/or health care providers have abandoned the legitimate
practices of science and have become anti-science activists.
Unfortunately, since many members of the public hold similar, very strong
beliefs about the same science-based issues (even though they don't have the
training or experience to personally evaluate decades of complex scientific
evidence), the anti-science activists can frequently find uncritical public
support for their opinions. Other
converts can be recruited by employing some of the tactics described below.
g.
The
consequences of ignoring science-based conclusions and resulting anti-science
actions by individuals with strongly-held, inflexible beliefs in their rights
and personal freedoms has probably never been demonstrated more obviously than
by the current pandemic.
Similarities of anti-science beliefs:
o
Ignoring the
scientific consensus that face mask use, social distancing and responsible
isolation limits the spread of viruses has led (and will continue to lead) to
the spread of the covid-19 virus.
o
Ignoring and
discounting the scientific consensus that
vaccinations limit the spread of viruses has led (and
will continue to lead) to the spread of communicable diseases.
o
Ignoring and
dismissing the scientific consensus that community water fluoridation is safe
and reduces the risk of tooth decay has led (and will continue to lead) to an
increase in dental decay and related health and social issues, particularly for
the disadvantaged.
2.
Fact
–
Community Water Fluoridation (CWF) is recognized a safe and effective public health measure by major and
respected science and health organizations worldwide, including in the U.S.,
Canada, Britain, Europe, Australia, New Zealand and other countries.
Health
agencies of all
50 states in the U.S. a
number of health insurance companies
and the States/Provinces in
Australia,
Canada and New Zealand also support CWF.
There are no
reputable science or health organizations that support the anti-F opinions. Bottom Line:
Trust The Experts!
![]() Click Here
For A List of Over 120 Organizations That
Support CWF
Click Here
For A List of Over 120 Organizations That
Support CWF
o
Lists of additional science/health organization that support CWF:
o
36 Reviews of
fluoridation studies
§
Again, if the FOs’ interpretation of the evidence is true, and the
mainstream science and health organizations that support CWF and other public
health measures like vaccination are
completely wrong, how can the mainstream organizations be trusted to provide
accurate information for any other science-based health issues?
3.
Fact –
Even mainstream science and health organizations that don’t
publicly endorse CWF do not post warnings against CWF or publicly state that CWF
causes any of the health issues claimed by FOs.
Specifically:
a.
Thyroid Problems – no warnings of thyroid risks from CWF:
o
American
Thyroid Association: No mention of fluoridation as a risk factor for
hypothyroidism
or
hyperthyroidism.
o
Australian Thyroid Foundation:
No mention of fluoridation as a risk factor for thyroid disorders.
o
Thyroid
Association of New Zealand: No mention of fluoridation as a risk factor for
thyroid issues.
o
British
Thyroid Foundation: No mention of fluoridation as a risk factor for
thyroid issues.
o
Thyroid UK
– No mention of fluoridation as a risk factor for hypothyroidism.
b.
Cancer Organizations – no warnings of cancer risk from CWF:
o
American
Cancer Society – Water Fluoridation and Cancer Risk: “The
general consensus among the reviews done to date is that there is no strong
evidence of a link between water fluoridation and cancer” and
“More recent studies have compared the rates of osteosarcoma in areas with
higher versus lower levels of fluoridation in Great Britain, Ireland, and the
United States. These studies have not found an increased risk of osteosarcoma in
areas of water fluoridation.”
o
Canadian
Cancer Society: “Based on
current evidence, CCS believes it is unlikely that adding fluoride to water
raises the risk of cancer, including osteosarcoma, in humans. At the same time,
we know that there are many benefits to water fluoridation, especially for
people who have less access to dental care. We will continue to watch this area
of research and update our information as we learn more.”
o
Cancer Council
Western Australia - Cancer myth: Fluoride and cancer: “Fluoridation
is considered by many to be a major public health achievement of the 20th
century. The addition of fluoride to drinking water has led to a significant
reduction in dental caries. There is no consistent evidence that fluoride in
drinking water increases the risk of cancer. The weight of the current evidence
supports the view that there is no link between water fluoridation and
osteosarcoma.”
o
Cancer
Society, New Zealand: “One hazard that has been mentioned is that
children drinking fluoridated water are at higher risk of developing an
extremely rare form of bone cancer called osteosarcoma.
At this time there is no evidence that this is true.”
o
National
Cancer Control Programme:
Water Fluoridation and effects on health:
“In conclusion, all systematic reviews to
date have found no association between fluoridation of drinking water at the
recommended levels and risk of cancer or bone fracture. The effects of fluoride
on health and related matters are kept under constant review. In addition, the
Expert Body on Fluorides and Health in Ireland is of the opinion that water
fluoridation significantly benefits dental health.”
o
National
Cancer Institute – Fluoridated Water: “More recent population-based studies using cancer registry data found no
evidence of an association between fluoride in drinking water and the risk of
osteosarcoma or Ewing sarcoma.” and in a DCEG article, Contaminants in
Drinking Water, stated “Over the years,
DCEG research on the association between contaminants in drinking water and
cancer has made a significant impact in the following areas:
A DCEG study found no evidence that fluoride in drinking water poses an
elevated risk of cancer, as had been suggested by some previous reports.”
c.
FOs resort to threats of legal action
against organizations that have publicly supported
CWF instead of working within the constraints of scientific protocol to present
legitimate evidence (if available) that could change the scientific consensus
that CWF is a safe and effective public health measure.
This constitutes a significant reason some health organizations have
removed their public endorsement of fluoridation.
If an organization is not directly responsible for dental health it can
be more prudent to remove an endorsement than risk a lawsuit.
The threatened groups, however, have not supported the
anti-fluoridation claims.
Several examples:
o
In 2016 a
threatening
letter to the American Thyroid Association prepared by
anti-fluoridation activist, Karen Spencer (who
created this letter), clearly exposes the anti-fluoridation
tactics. The petition ‘suggests’
the ATA “Publish a position statement opposing the practice of community
water fluoridation…” and provides a not-so-subtle suggestion of potential
consequences of ignoring the petition, “In
closing, given the fluoridation lawsuit pending in Peel, Ontario … and
other anticipated American lawsuits yet to be filed, we
suggest that the ATA leadership and directors should be prepared to
demonstrate their scientific integrity and professional ethics. We suggest the
ATA speak for themselves…”
o
In 2015 a
letter threatening legal action
if the
anti-fluoridation agenda was not
followed was sent to the National Academy of Sciences, Institute of Medicine
(NAS/IOM) –– now the National Academy of Medicine –– board members, “Failure to address
the current fluoride DRI and assertions in NAS/IOM reports regarding safe levels
of fluoride for pregnant women, fetuses, young children, the elderly, and those
with health conditions or a genetic profile that increases their susceptibility
as noted in this document with parties using that material in the making of
individual and public health decisions may result in legal action.”
o
In 2007
anti-fluoridation attorney,
Robert Reeves, sent the National Kidney Foundation (NKF) a
threatening letter
suggesting potential lawsuits against the then current and past members of the
NKF Board of Directors, both collectively and against their personal assets, as
well as against the NKF staff, if NKF did not remove its name from the list of
organizations which support fluoridation – “In
light of your mission of educating and empowering kidney patients, to not openly
inform the kidney patient community of the whole story about fluoride is
actionable under a number of legal mechanisms for enjoinder ,suit and negligent
misrepresentation. … Even if it is ultimately determined that neither NKF or any
past and present Officers, Board Members and/or employees are liable criminally
or for any tort such as negligent misrepresentation this still could be a major
public relations disaster for NKF which is best handled now rather then later..” The NKF
is a charitable organization which provides much needed services and activities
on behalf of kidney patients. Rather than waste its limited resources and
subjecting its Boards and staff to protracted and expensive litigation fighting an
antifluoridationist attorney with nothing to lose, the NKF prudently decided to
simply remove its name from the list.
Review the
reference to AWWA/NKF
threat discussed above.
o
Question to consider:
Why are threats of legal action necessary if the arguments and opinions
presented in these threatening letters are a legitimate and accurate
representation of the actual scientific evidence?
§
Do members of these organizations simply ignore widespread claims that CWF is
dangerous &/or are they too lazy or dumb to evaluate or understand any new
evidence?
§
Have the members actually determined fluoridation is harmful but have decided to
ignore the issue and keep recommending a harmful practice for some reason and
just let their patients and fellow citizens suffer?
§ Or –– perhaps there is no legitimate, persuasive evidence to support the anti-fluoridation claims - that's my choice!
4.
Fact –
In stark contrast to the widespread
support for CWF by respected science and health organizations worldwide
–– and the hundreds of thousands of scientists and health professionals they
represent –– I am aware of no
major, recognized science or health organizations that have publicly stated CWF
is harmful or ineffective, and there are relatively few scientists and/or
health care providers that support the anti-fluoridation conclusions.
** In fact, I have only found a few alternative
science/health organizations that accept the anti-fluoridation
opinions as legitimate. The few I have found that
promote a public anti-fluoridation policy are
listed below. These organizations
often also subscribe to other ‘medical’ notions that don’t conform to mainstream
medical practices.
![]() Additional
Details Here
Additional
Details Here
5.
Two extremely important questions to consider based on the above facts:
If the arguments and claims of FOs are a scientifically accurate
interpretation of the evidence and are presented correctly, fairly and
truthfully:
a.
Q1 – Why do the major science and health organizations in the world
(and the hundreds of thousands of members they represent) continue to support
CWF and not the anti-fluoridation opinions?
b.
Q2 – Why do only a relatively small number of trained and experienced
scientists &/or medical professionals support the anti-fluoridation agenda and
beliefs?
·
My Answer:
The decision to dismiss the interpretation of available evidence
supporting a scientific consensus that is accepted by most scientists in the
world requires trusting in one’s strongly-held, inflexible beliefs instead of
the relevant scientific consensus.
That conviction demands requiring that the evidence be selected, interpreted and
presented to support those beliefs.
As noted previously, in order to change a scientific
consensus, legitimate new scientific evidence must be presented to experts in the
relevant scientific community sufficient to initiate change.
For over 70 years, FOs have been
completely unable to provide a single confirmed, convincing, legitimate,
reproducible, scientific study to support their claims that drinking optimally
fluoridated water is ineffective or harmful to health
– that includes recent F–/IQ studies aggressively promoted by FOs.. The scientific
consensus that fluoridation is safe and effective has not changed.
The arguments and claims of FOs are not based on an impartial, accurate
&/or truthful representation of the 75-year body of scientific evidence.
6.
Another critical question to consider: Since there are only a
relatively few scientists and health professionals, virtually no mainstream
scientific organizations, a few alternate health groups and some questionable
supporters of the anti-fluoridation arguments that CWF is dangerous and
ineffective –– and it can be easily demonstrated that the available
ant-fluoridation ‘evidence’ is presented inaccurately –– how is it possible that
FOs are often successful in their efforts to ban or stop community water
fluoridation?
a. My Answer: FOs (and others who oppose widely-accepted science-based conclusions) are extremely dedicated, vocal and persistent in their mission to end CWF (or challenge other accepted science-based conclusions). There are a number of often successful tactics employed by FOs and other anti-science activists to “adjust” public opinion and encourage members of a community to actively and vocally oppose an accepted scientific conclusion.
7.
Fact: The
anti-science tactics
employed by FOs (and others
who dismiss an established scientific consensus) to try and convince members of
the public to trust their proclamations that CWF is dangerous, unethical and
ineffective over the conclusions of mainstream science and health professionals
must be exposed so they can be understood
and dismissed by rational, caring members of the public:
a.
As described earlier, FOs completely
ignore the scientific consensus if possible, dismiss it as an irrelevant
farce if confronted with it and avoid working within the scientific community to
provide legitimate scientific evidence (which does not exist) necessary to
change the consensus.
b.
FOs Hijack the
Democratic Process:
Democracy
only works if good decisions are made by accurately informed members of the
public –– whether they are the voters making decisions that determine how
science is used to best help and protect their fellow citizens or the
individuals elected by the voters who are entrusted with making those
science-based decisions. Since most of the voters and elected officials are not
trained scientists or health care professionals, it is the goal of anti-science activists to generate distrust of any
scientific consensus they disagree with and the scientists and/or health care
providers who support the consensus of relevant experts.
Since the ‘evidence’ of
anti-science activists is not sufficient to convince the majority of relevant
experts to change the scientific consensus, FOs must take their battle against
science directly to the public, confident that most individuals will not try (or
be able) to understand the science.
Anti-science activists argue that the concept of a scientific consensus is
irrelevant. They try to replace it
with a public consensus where
conclusions based on complex scientific evidence can be determined (and voted
on) by anyone (based on their beliefs), regardless of training and experience,
instead of by scientists and health care professionals who actually understand
the evidence and its context and the consequences of making science-based
decisions.
Many well-meaning members of the public are persuaded by the anti-science
arguments, and they choose to unconditionally trust the anti-F–
conclusions on CWF over those of mainstream scientists and health professionals.
These converts make up the FOs’ militia, and they are directed to vocally
oppose CWF in their communities by attending community meetings and voicing
their opinions voting for (or adopting, if they are elected officials) anti-F–
policies. The same tactics are used
by vaccination opponents.
c.
FOs Employ Fear Mongering
to Try and Change Public Opinion and Spread Discord:
Fear is an
extremely powerful motivator of public opinion, and FOs exploit the complexity
of fluoridation science and the power of fear to drive their anti-science,
fear-mongering campaign.
FOs try and convince concerned citizens that a
beneficial public health measure is actually evil incarnate.
FOs can effectively dispense their shock and scare content because they
bypass normal channels of scientific review and deliver their message directly
to the media and the public.
It is far easier to create and promote negative, fear-invoking ‘evidence’
than it is for most scientists and health care workers to provide and discuss
accurate, complex scientific evidence to refute the fear-based claims.
Part of the problem is that exposure to excessive levels of fluoride ions
(way above those found in CWF) can cause negative health issues – just like
excessively high exposure to other substances.
Examples:
·
“Fluoride
is a deadly poison”
sounds really scary – who in their right mind would want to drink
water that contains a deadly poison.
This simple claim is far more effective at manipulating public opinion
than trying to describe the science-based fact that low levels of fluoride ions
in optimally fluoridated water (0.7 ppm) are safe and actually protect health.
·
"Due to its high toxicity,
fluoride has long been used as a pesticide. In the United States, there are
currently two fluoride-based pesticides that are allowed to be sprayed on food.
These are: cryolite and sulfuryl fluoride." &
“Sodium Fluoride used in Rat Poison. While
it’s one of the main ingredients in toothpaste, sodium fluoride is widely used
in rat and cockroach poisons.”
It should be apparent that the use of fluorine in pesticides or rat poison has
absolutely nothing to do with CWF.
Chlorine is also used in pesticides.
By the ‘logic’ of FOs, water disinfection and salt should be banned.
The fact is, virtually any substance is a deadly poison at high enough exposure
levels – even drinking
too much water
can be a
deadly poison.
FOs completely ignore the concept of dose (or exposure level), because an
accurate statement that too much fluoride exposure (drinking water with 3-4
times more than the optimal level of fluoride) can increase the risk of dental
fluorosis would not cause anyone to take notice of their claims.
·
“Fluoride is a
highly toxic substance that can cause a range of adverse health effects.”
CWF reduces IQ, and studies prove CWF causes
ADHD, other neurological problems, arthritis, bone fracture, cancer,
cardiovascular disease, diabetes, GI effects, hypersensitivity, kidney disease,
male fertility and pineal gland issues, skeletal fluorosis and thyroid disease.
These claims sound
really scary – who in their right mind would want to drink water that severely
damaged one’s health?
Compare those horrifying claims with the science-based conclusions that, in over
75 years of studies, drinking optimally fluoridated water has not been shown to
cause any health issues besides lowering the risk of dental decay by 15% - 25%
or so. Which of these claims is more
likely to cause someone to take action if they accepted it as true?
(discussed below)
·
CWF is a “Toxic
Treatment:
Fluoride’s Transformation from Industrial Waste to Public Health Miracle. …
unlike the pharmaceutical grade fluoride in their toothpaste, the fluoride in
their water is an untreated industrial waste product, one that contains trace
elements of arsenic and lead.”
Sounds really scary, right? These
claims are often a strong motivation for fear that trumps the science-based
description that many fluoridation chemicals are a byproduct of processing
phosphorite rock
and are carefully regulated so contaminants are nearly undetectable and
certified to be within safe limits.
“In
fact,
NSF
was only able to detect the reported trace amounts [of contaminants] by dosing
the chemicals into reagent water at 10 times the manufacturer’s maximum use
level.”
Additional information.
·
**
As stated previously, how can someone who is not trained and experienced in
science &/or health care determine which claims are true?
Will a significant number of people make the effort to find and try to
understand the scientific evidence, or will they simply confirm the fearful
claims with a Google search?
d.
FOs Employ
Gish Gallop: Another very common
tactic of anti-science activists is Gish Gallop, “a
technique used during
debating
that focuses on overwhelming an opponent with as many arguments as possible,
without regard for accuracy or strength of the arguments. The term was coined by
Eugenie Scott
and named after the
creationist
Duane Gish,
who used the technique frequently against proponents of evolution.” (Wikipedia)
“By
using a quantity of arguments as a quality itself, a
Gish Gallop
tries to create the illusion of authority and weight of evidence. It is
effectively
style over substance.”
“A
Gish Gallop is a well-established method of outmaneuvering rhetorical opponents
with an overwhelming onslaught of dubious arguments. The Gallop works by
leveraging two basic tendencies in human reasoning. First, it’s easier and
faster to make a false claim than it is to disprove one.
Second, if an opponent fails to disprove every single one of the spurious
statements you state, you can claim victory on the leftovers.” (Carl Alviani).
(Pseudo-)Science
Blog,
Effectivilolgy,
Skeptical Science,
Open Parachute).
I discussed one example,
James Reeves,
earlier.
·
One of the
most remarkable examples of Gish Gallop I have experienced was a series of posts
by Bill Osmunson trying to link fluoridation and cancer.
In the posts Osmunson dumped over 16,000 words (referencing over 80
studies) into the exchange in an apparent attempt to support his claim that
drinking optimally fluoridated water is a significant risk factor for causing
cancer:
“Randy, Lets talk science rather
concensus. Remember, the masses can
be wrong. Marketing can change
public opinion. The next few posts
will be just a touch on one aspect of fluoride, carcinogenicity.” (09-04-2018
02:04 PM),
“Randy, Let’s look at some studies.” (09-04-2018
02:05 PM),
(09-04-2018 02:07 PM), (09-04-2018
04:11 PM),
(09-04-2018 04:12 PM), (09-04-2018
04:47 PM),
(09-04-2018 04:57 PM), (09-04-2018
05:02 PM),
(09-04-2018 05:03 PM), (09-04-2018
05:05 PM),
(09-04-2018 05:06 PM), (09-05-2018
04:12 PM),
(09-05-2018 04:14 PM), (09-05-2018
04:18 PM),
“This forum only accepts 20,000
charactors, so I cannot post all the fluoride cancer studies.
Here are some, in response to your claim, ‘Fluoride is NOT a carcinogen’”
(07-11-2018
06:26 PM)
(Note:
The site changes, and it may be necessary to go back or forward a page
or so.)
My response – I asked
Osmunson, if he had all of that legitimate evidence proving CWF caused cancer,
why did he present it in a public forum instead of demanding a meeting with
cancer experts to demonstrate why his evidence should be sufficient to change
the scientific consensus. He
provided no answer. If you examine
other comments From Dr. Hanie and David Fierstien asking specific questions of
Osmunson regarding his claims, they were also unanswered.
If any of the anti-fluoridation
interpretations of the studies were legitimate, why do none of the cancer
organizations list community water fluoridation as a cancer risk?
Do the activists have a better understanding of the evidence than the
relevant experts? Why would anyone
trust the opinions of passionate activists who have no legitimate training or
evidence to support their opinions, but who continue to dump tons of irrelevant
studies into public discussions.
e.
FOs claim
accidents with some link to fluorine happen, so CWF should be banned:
·
A report on the Fluoride
Alert site stated, "Marin County – October 26 – November 1, 1977.
Fluoride feeder valve malfunctioned. Five communities received fluoride above
'accepted' level for several days without notice to the public."
Other accidents were listed as well.
Following the logic of this argument, chlorination of drinking water
should be banned because accidents occasionally occur that release chlorine
compounds into the environment and kill or injure people.
So, everyone should be responsible for the disinfection of their own
water.
Perhaps every human activity in which
accidents occur should be banned.
·
A headline from Fluoride Alert
screamed, "Reported Poisoning Incidents from Fluoride Toothpastes, Supplements,
& Mouthrinses: As a result of the FDA’s warning, there are now over 20,000
reports each year to Poison Control Centers in the United States due to
excessive ingestion of fluoride toothpaste."
·
Child’s death – a tragic
accident, but completely unrelated to CWF.
·
3 Hemodialysis
patients died – tragic, but related to
equipment
failure,
unrelated to CWF.
·
“A
blast at the factory of chemical maker Hube Global on September 27th killed
five people and led to the leakage of EIGHT tons of hydrofluoric acid.”
Of course
hydrofluoric acid production has absolutely nothing to do with the safety
and effectiveness of CWF, but that doesn’t stop FOs from trying to spread fear.
o
It is completely irresponsible, irrelevant and disingenuous to use unfortunate
accidents that have nothing whatever to do with CWF to try and "prove" drinking
optimally fluoridated water is harmful.
Think of what would happen if every activity that could be linked (even
remotely) to an accident was banned.
This is one of the more irrational anti-F tactics.
f.
FOs “Create A
Veneer of Science to enhance the appeal of their claims”: FOs (like all anti-science
activists) conduct questionable studies, reference (cherry-pick) poor quality
studies, inconclusive studies &/or studies that are irrelevant to CWF as 'proof'
their opinions are valid, and they deliberately distort conclusions of
legitimate scientific evidence before spinning it out to the public. The
fact is, any study allegedly supporting the anti-fluoridation opinions that
fluoridation is harmful will have one or more of the following characteristics:
1.
The study
referenced had nothing to do with drinking optimally fluoridated water.
Examples:
o
 “Developmental
fluoride neurotoxicity: a systematic review and meta-analysis: Choi, Zhang, Grandjean, 2012” was one of the first reviews utilized by FOs to scare people
into fearing CWF lowers IQ. It was
promptly criticized by scientists and health professionals because the studies
reviewed had absolutely nothing to do with CWF, had low sample sizes and high
fluoride levels, didn’t consider other contaminants and risk factors and had
other significant limitations. The coauthors even admitted “each of the articles reviewed had deficiencies, in some cases rather serious ones,
that limit the conclusions that can be drawn.”
Critique 1,
Critique 2,
Critique 3,
2013 response of CWF support from Harvard Deans.
“Developmental
fluoride neurotoxicity: a systematic review and meta-analysis: Choi, Zhang, Grandjean, 2012” was one of the first reviews utilized by FOs to scare people
into fearing CWF lowers IQ. It was
promptly criticized by scientists and health professionals because the studies
reviewed had absolutely nothing to do with CWF, had low sample sizes and high
fluoride levels, didn’t consider other contaminants and risk factors and had
other significant limitations. The coauthors even admitted “each of the articles reviewed had deficiencies, in some cases rather serious ones,
that limit the conclusions that can be drawn.”
Critique 1,
Critique 2,
Critique 3,
2013 response of CWF support from Harvard Deans.
o
One of the first studies in Osmunson’s fluoride/cancer Gish Gallop example above
(Pal S, Sarkar
C, 2014) exposed rats to “sodium
fluoride at a dose of 20mg/kgb.w./day for 30 days” and found it caused serious
health issues.
Ok, let’s put that into a rational perspective.
That’s the equivalent of human exposure of 1.8 mg F–/kgb.w./day.
That would require a 4.5 Kg (10 pound) infant to ingest 8.1 mg of
F– per day by drinking 11.6 liters
(3 gallons) of optimally fluoridated
water. A 150 pound adult (68 Kg)
would have to ingest 122 mg F– per
day by drinking over 85 liters (22
gallons) of optimally fluoridated water per day.
Of course high exposure levels to most
any substance can cause harm – think of what would happen if infants consumed
3 gallons of water per day!
It should be obvious that results from this study have nothing to do with
CWF, but that doesn’t stop FOs from using studies like this to try and ‘prove’
CWF causes cancer. FOs don’t care
about honesty, accuracy or relevance – only about creating fear.
2.
The study
examined exposure to fluoride ions at far higher levels than found in optimally
fluoridated water. (Examples below)
3.
The study
conclusions may suggest a possible correlation (or association) between two
variables, but that does not prove a cause and effect relationship.
4.
The study
didn’t consider or adjust for numerous other factors potentially associated with
the alleged risk, and it proved nothing.
5.
The study was
unrepeatable by other legitimate, impartial scientists.
6.
The study
methodology was demonstrably flawed and had significant limitations.
7.
The study
conclusions are contradicted by the majority of related studies
&/or
8.
The claim was
a complete fabrication.
Unfortunately, without diving into the complexities of each of the hundreds of
studies cited by FOs to support their opinions, it is difficult to prove the
claims above are true. I will
provide some specific examples below to illustrate the tactics, but my examples
only expose the most basic and obvious limitations of the studies – these
explanations don’t begin to explain in detail the specific, serious limitations
of the each of the studies that have caused the scientific community to reject
them as legitimate evidence that CWF causes harm.
·
These are
examples of characteristic 2 above: These are also
examples of the complexity of actually trying to evaluate the scientific
literature and explaining the results – even if one is a scientist.
It is important to understand that in rats, “a
5-fold
increase in the dose of fluoride ions is required to achieve comparable human serum
levels.”” (FiDW p 98)
So, to approximate an optimal level of fluoride (0.7 ppm or mg/L) from
CWF, a rat would have to drink water containing 3.5 ppm F–,
and rats drinking water containing 20 ppm F–
would be equivalent to a human regularly drinking the EPA maximum contaminant
level (MCL) of 4 ppm F– or 4 mg/L.
o
Neurotoxicity of sodium fluoride in rats – “Weanlings
received drinking water containing 0, 75, 100, or 125 ppm F for 6 or 20 weeks,
and 3 month-old adults received water containing 100 ppm F for 6 weeks.”
The lowest exposure level in this study (75 ppm) was 3.75 times higher
than the EPA’s MCL of
4 ppm, human (20 ppm rat) and the highest level was 35.7 times greater
than optimally fluoridated water (0.7 ppm human / 3.5 ppm rat equivalent)
o
Roles of
mitochondrial fission inhibition in developmental fluoride neurotoxicity – “uusing Sprague-Dawley rats
developmentally exposed to NaF (10, 50, and 100 mg/L [that’s 4.5, 22.5 and 45
mgF–/L] from pre-pregnancy until 2 months of delivery to mimic human exposure…”
Actually, the study doesn’t mimic human exposure to CWF.
The lowest level (4.5 mg/L) is higher than the optimal level in CWF, 22.5
mg/L is higher than the EPA MCL, and 45 mg/L is over 10 times
higher than the fluoride content of optimally fluoridated water.
How many substances do you think could be demonstrated to have harmful
effects at 10 times the recommended exposure level??
o
–>
Contrast the above studies with a 2018 Study,
An Evaluation of Neurotoxicity Following Fluoride Exposure from Gestational
Through Adult Ages in Long-Evans Hooded Rats,
designed and conducted by the NTP to evaluate potential harm of fluoride
concentrations at levels 2.5 to 5.7 times that found in optimally fluoridated
water (0.7 ppm). “Long-Evans
hooded male rats maintained on a standard diet (20.5 ppm F−)
or a low F−
diet (3.24 ppm F−)
with drinking water exposure to 0, 10, or
20 ppm F−
from gestational day 6 through adulthood. … Equivalent human daily water intakes
of 1.74 mg F/day for an adult or 0.63–1.23 mg/day for 1 to 14 years of age have
been approximated in rodents using drinking water concentrations of 7 to 9 ppm F−.
In the current study, the top dose of 20 ppm F−
was selected based upon the US Environmental Protection Agency’s Maximum
Contaminant Level of 4 ppm [5.7 times higher than optimally fluoridated water]
and the conventional wisdom that a 5-fold increase in dose is required to
achieve comparable human serum levels.
Conclusions:
“At these exposure levels, we observed no exposure-related differences in
motor, sensory, or learning and memory performance on running wheel, open-field
activity, light/dark place preference, elevated plus maze, pre-pulse startle
inhibition, passive avoidance, hot-plate latency, Morris water maze acquisition,
probe test, reversal learning, and Y-maze. Serum triiodothyronine (T3),
thyroxine (T4), and thyroid stimulating hormone (TSH) levels were not altered as
a function of 10 or 20 ppm F−
in the drinking water. No exposure-related pathology was observed in the heart,
liver, kidney, testes, seminal vesicles, or epididymides.
Mild inflammation in the prostate gland was observed at 20 ppm F−.
No evidence of neuronal death or glial activation was observed in the
hippocampus at 20 ppm F−.”
As NTP researchers were preparing to conduct this study, FOs praised the
NTP and were confident this “New
Fluoride/Brain Study Could End Fluoridation”
·
Several recent
studies (2017 Bashash
et al.
and
2019 Green, et
al.)
are heavily promoted by FOs as proof that CWF reduces IQ, yet they
provide excellent examples of
characteristics 3, 4, 5, 6, 7 and 8 above.
In fact, these studies were so obviously flawed they received immediate,
significant and detailed criticism from relevant experts worldwide. (Green1,
Green2,
Bashash1,
Bashash2,
G&B
Unfortunately, many well-meaning citizens who don’t have significant science
&/or health training can easily be scared by fluoridation opponents (and
irresponsible journalists) who present these studies as convincing evidence
fluoridation causes lower IQ .
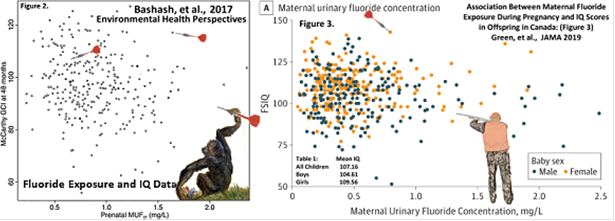
However, anyone with a moderate understanding of science (and no prior anti-F–
bias) can examine the graphs presented in the articles and realize the
importance of two statistical facts that cast immediate doubt on any conclusions
made by the authors (or other FOs) that CWF might lower IQ:
1. A correlation (or association)
between variables
does not imply
a cause and effect relationship.
2. The
greater the
scatter of data points in a graph, the weaker any potential correlation will be.
They will then conclude that any conclusions based on that data will be highly
suspect.
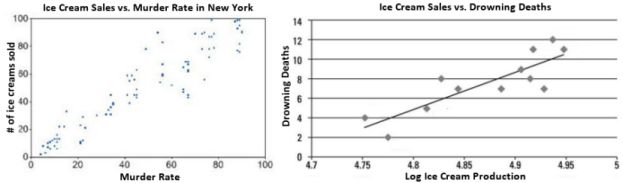
An example: The two graphs above
show strong
correlations
between ice cream sales and deaths and would provide anti-ice-cream activists very strong evidence
that Ice Cream Consumption is Dangerous
and All Sales Should Be Banned.
Hopefully it is obvious there might be other variables involved (like
temperature) that have not been included in the analysis, but are more likely to
correlate with death rates than ice cream sales.
This example is just one relatively simple illustration of the many ways
anti-science activists can produce study results that appear to support their
opinions.
The dependence of FOs (and all anti-science activists) on the way their
so-called ‘evidence’ is produced, packaged and promoted (as described above) is
the primary reason they have been
completely unsuccessful in changing the scientific consensus –
unfortunately, it is also the reason they have often been successful at
influencing public opinion.
For anyone who trusts the majority of scientists and health professionals, the
best argument that the ‘evidence’ provided by FOs should not be trusted is that
no mainstream science or health organizations accept any of the studies
referenced by FOs as valid, significant evidence CWF is harmful or ineffective.
g.
FOs Blur the Boundary Between Ethics and Science to Fabricate False Moral Arguments:
For example, FOs portray CWF as a medication that constitutes an immoral
violation of one’s personal freedom by forcing a medication on unwilling members
of the public. Specific example
FAN claims
that, “Unlike all other water treatment processes, fluoridation does not
treat the water itself, but the person consuming it. The Food & Drug
Administration accepts that fluoride is a drug, not a nutrient, when used to
prevent disease. By [FOs'] definition, therefore,
fluoridating water is a form of mass medication.” That opinion is not science – it’s not
even a supportable belief – yet it fuels the chaos FOs promote.
Fact: The claim that “The FDA accepts that fluoride is a
drug” is spurious, because the
FDA does not regulate water treatment chemicals, and the FDA does regulate
fluoridated bottled water as a “Food
For Human Consumption”, not a drug. If the FDA regulated fluoridated
bottled water as a drug, warnings similar to those on toothpaste (which contains
fluoride levels over 1,000 times greater than optimally fluoridated water) would
be required to have warnings. FOs can reference no regulations that CWF
constitutes any form of medication from any source besides their own opinions.
The FAN claim, “Unlike all other water treatment processes, fluoridation does
not treat the water itself, but the person consuming it.” is an example of how
reality can be ‘adjusted’ to fit a specific
·
The argument that there is a difference between treating the water
vs. treating the person is completely irrelevant and misleading.
Fact:
All elements/chemicals that impact human health (either
positively or negatively) “treat the
person”. Although some chemicals
like lead “treat the person” poorly at
any exposure level, many elements/chemicals “treat
the person” positively at low to moderate exposure levels and negatively at
excessively high exposure levels.
For example, while sodium, potassium, chlorine, vitamins, calcium, H2O, etc. are
beneficial at low appropriate exposure levels, they are all deadly poisons at
excessively high exposure levels.
It is remarkable that the concept “The Dose Makes
the Poison” was understood nearly 500 years ago, but the FOs completely
ignore the concept, claiming that
Fluoride is a deadly poison without any context of exposure levels – and completely contrary
to the 75-years of scientific evidence that has demonstrated low-level exposure
to fluorine is beneficial to health.
** This is one of the better examples of how the presentation of accurate facts in a deliberately misleading manner can scare concerned, well-meaning individuals into signing a
petition to ban dihydrogen monoxide (more DHMO facts) Think of what can be accomplished if individuals, in their passion to change public opinion, are not constrained by an obligation to present information accurately and responsibly.
·
All water treatment methods involve adding chemicals that are
toxic at high levels to the water.
Disinfection also creates
disinfection byproducts
like
chloroform
which are also harmful at high exposure levels and have no health benefits.
It is irrelevant whether you arbitrarily label them a medicine, a poison,
or a treatment chemical.
·
Using anti-science arguments one could create a case against drinking water
disinfection by claiming “Unlike all other water treatment chemicals
chlorine has been used as a chemical weapon, and the disinfection byproducts do
not treat the water itself, but, like the element chlorine, pose a threat to the
person consuming it. The CDC recognizes
chlorine
is poisonous, and DBPs as potentially
causing liver
damage and decreased nervous system activity. By definition, therefore,
water disinfection is a form of mass poisoning and should be abandoned.”
Take a look at the EPA
Risk Assessment of Disinfection Byproducts (DBPs),
there is no evidence that exposure to DBPs (or the disinfectants) treat the body
in a beneficial manner: “EExposure to DBPs is a potential human health hazard; both the
epidemiologic and toxicologic literature provide some evidence of potential
adverse health effects. Taken as a whole, epidemiologic studies on chlorinated
drinking water offer some evidence of an association with certain cancers,
reproductive and developmental effects, warranting further investigation.
…
In in vivo studies at high doses of individual DBPs and some defined
DBP mixtures, there is evidence of carcinogenicity,
reproductive and developmental effects, nephrotoxicity and hepatotoxicity.”
Note: I am in no way endorsing these
arguments, only demonstrating how facts can be manipulated to create a
fear-based ‘moral argument’. In
fact:
o
CWF and other water treatment processes (disinfection, pH adjustment, corrosion
control and flocculation/coagulation) all protect the health of citizens who
drink the water by different methods – reducing dental decay, killing pathogens,
removing contaminants, reducing the risk of harmful chemicals leaching from
pipes, etc.
o
The benefits of all drinking water treatment methods to protect the health of
the entire population far outweigh any risks, and the chemicals which remain in
the treated water are regulated to be within safe limits. Take a look at your
water quality report – there are low but safe amounts of a number of potentially
harmful chemicals in all public water.
h.
FOs Employ the Freedom of Choice Argument and claim CWF constitutes forced mass
medication
(or intentional poisoning) –– Anyone drinking public water should have a choice
regarding any chemicals they are exposed to.
This is a legitimate argument for individuals deciding on personal exposure to
substances that are not part of public health measures (like vaccination
programs and water treatment processes) that impact entire communities – not
just individuals.
References: (Open
Parachute,
Fluoridation Facts, p 92)
i.
FOs Claim Most of the World doesn’t Fluoridate their Water & Decay Rates Have
Fallen Both in Countries that use CWF and Those that Don’t.
This is another example of the selective presentation of actual evidence.
·
Claim: Most of the Countries in the World
don’t Fluoridate their Water.
It is true most countries don’t employ CWF, but the reasons are not based
on scientific evidence that fluoridation causes harm
or is ineffective. Reasons for not
utilizing CWF include sufficient natural fluoride levels, lack of centralized
public water supplies, utilization of fluoridated salt or milk, and other
technical, legal, financial or political reasons (Fluoride
Facts, p 102,
Fact *13,
Skeptic,
CDHP,
PEW)
·
Claim: Decay Rates Have Fallen Both in
Countries that use CWF and Those that Don’t.
FOs often present several graphs allegedly showing that over the last 45 years
or so decay rates
have decreased in countries that employ CWF and those that don’t.
The article “Is
Fluoridated Drinking Water Safe””
by Nicole Davis (with comments by P. Grandjean) in the Magazine of the Harvard
T.H. Chan School of Public Health demonstrates a common example of how
information can be misrepresented – and yet appear legitimate.
The story received significant and very specific criticisms from
Oral Health Representatives of the UK and Ireland
the presidents of the
AAP
and
ADA,
including requests for recension/retraction from the
Dean of Harvard School of Dental Medicine
and
members of the Harvard School of Dental Medicine and
several alumni of the Harvard School of Public Health.
The criticisms clearly demonstrate how
Nicole Davis utilized the
anti-science tactics outlined above.
·
Facts:
The graphs presented by FOs to try prove CWF is ineffective are
country-wide and fail to consider/compare fluoridated vs. non-fluoridated
communities, natural F—
levels, or take into account other
methods utilized to reduce decay in different communities.
A
detailed discussion
of how graph data is misrepresented by FOs.
Other examples:
o
In a
recent study,
July 2020, from New Zealand concluded, “In
this national cross-sectional study of 275,843 children, those living in areas
without community water fluoridation had significantly higher odds of severe
caries compared with children living in areas with water fluoridation after
adjustment for age, sex, ethnicity, area-level deprivation, and residual
location.”
o
Most studies have demonstrated an increase in decay rates after stopping
fluoridation in communities which did not make any other recorded changes to
oral health risk factors:
Does cessation
of community water fluoridation lead to an increase in tooth decay? A systematic
review of published studies: McLaren &Sonica Singhal, J Epidemiol Community
Health. 2016 – “Overall, the published
research points more to an increase in dental caries post-CWF cessation than
otherwise.”
o
Three recent studies have demonstrated an increase in dental decay in cities
after CWF was halted:
~>
Juneau, AK
–
Consequences of community water
fluoridation cessation for Medicaid-eligible children and adolescents in Juneau,
Alaska: Jennifer Meyer, et al., BMC Oral Health201818:215, “Additionally,
the age group that underwent the most dental caries procedures and incurred the
highest caries treatment costs on average were those born after CWF cessation.” (Discussion)
~> Windsor, Ontario –
City Council voted to remove CWF in 2013 and
reintroduce it in 2018. The
Oral Health Report 2018 Update, Windsor-Essex County Health Unit: “From
2011/2012 to 2016/2017, communities that recently ceased fluoridation observed a
greater decrease in the percentage (13%) of students without caries compared to
an 8% decrease in the communities that were never fluoridated.”
~>
Calgary,
Alberta –
Measuring the short‐term
impact of fluoridation cessation on dental caries in Grade 2 children using
tooth surface indices: Lindsay McLaren, et al., Community Dentistry and Oral
Epidemiology, June 2016: “Trends
observed for primary teeth were consistent with an adverse effect of
fluoridation cessation on children's tooth decay, 2.5–3 years post‐cessation.
Trends for permanent teeth hinted at early indication of an adverse effect.”
o
It is true most countries don’t employ CWF, but the reasons are not based on
scientific evidence that fluoridation causes harm or is ineffectiveness.
Reasons for not utilizing CWF include sufficient natural fluoride levels,
lack of centralized public water supplies, utilization of fluoridated salt or
milk, and other technical, legal, financial or political reasons (Fluoride
Facts, p 102,
Fact *13,
Skeptic,
CDHP,
PEW))
j.
FOs Make Public, Libelous Claims
against the scientists and health care professionals who disagree with them,
sowing confusion and encouraging public distrust of the scientific processes and
the science and health communities.
** To convince the public their opinions are valid,
FOs claim those who support CWF are either too stupid or incompetent to
understand and recognize evidence FOs claim proves obvious dangers of
fluoridation. Or they may claim all the
pro-CWF professionals actually understand the issue but simply don’t care about
the alleged havoc fluoridation is causing to the health of their families and
fellow citizens – or they are being paid by some mysterious
“fluoride-conglomerate” to keep silent.
** Since the scientific evidence does not support their strongly held,
inflexible opinions, FOs try and convince concerned citizens that a beneficial
public health measure is actually evil incarnate supported by a bunch of
ignorant fools. A primary argument
is that representatives of all supporting science/health organizations are
either too stupid or incompetent to understand and recognize what FOs claim are
obvious dangers of fluoridation.
Another anti-F– explanation is
that professionals who support CWF actually understand the dangers, but they
simply don’t care about the alleged havoc fluoridation is causing to the health
of their families and fellow citizens.
Examples:
·
Anti-fluoridation activist Bill Osmunson, DDS, MPH provides the following
explanations for why the mainstream science and health organizations continue to
support CWF:
(07-09-2018 9:09
PM)
“CDC references the ADA and AAP, and the ADA and AAP reference each other
and the CDC. Circular referencing.
.. Johnny, the credibility of those so called "scientific" organizations has
been seriously tarnished. They do
not protect the public.
They are lemmings, followers, part of a
herd, not scientists. Scientists
question and do not assume and base their science on trust. Those allegedly
"credible" scientific organizations promoting fluoridation at 1 ppm have not and
did not review the science and follow the
science. [note, when this was written, the accepted fluoridation level was
actually 0.7 ppm] They all waited
for someone else to stand out from the herd and protect the public. … They were
silent because they never looked at the science” and on 8/19/2018 stated, “The
CDC simply reacts to the ADA and they don't think for themselves or review the
research.
CDC does not determine the dosage, efficacy or safety of any substance
used to prevent disease.”
(Note:
The site changes, and it may be necessary
to go back or forward a page or so.)
·
Another anti-fluoridation activist, posting under the name “CarryAnne”
(her background history and arguments match anti-fluoridation activist,
Karen Spencer
– the author of
threatening letters
to health organizations) provides the following explanations for why the
mainstream science and health organizations continue to support CWF:
(08-22-2018
06:59 AM)
“Willful blindness and financial
benefit affect both organizations
[ADA and EPA] and individuals and are eminently rational rationales for refusal
to change, although also morally corrupt”
and ”vested interests are doing their part
to protect a profitable program that
causes misery to millions” and ”Agnotology: Culturally induced
ignorance or willful blindness, particularly the promotion of misleading
scientific data and anecdotes by a biased group”
(08-19-2018
01:05 PM)
that, “I don't believe most dentists intentionally support fluoridation for
this purpose [big bucks earned from treating dental fluorosis].
Most are either ignorant or willfully blind. Others are either
cowed into silence per my previous comments or are indeed
sociopaths motivated by power,
prestige and paychecks”
(07-25-2018
11:30 PM)
“the malignant medical myth of
fluoridation persists because not only is there a profitable business model
built on fluoridation, fluoridation
promotion is profitable to many advocates”
(07-03-2018
07:35 AM)
“I have it on good authority that they [American Thyroid Association]
don't want to provoke a political storm with other groups - cowards."
The site changes, and it may be necessary
to go back or forward a page or so.)
A reminder that it isn’t
just a few marginal science and health organizations that support CWF – as noted
above, the overwhelming majority of respected, mainstream organizations support
CWF. Is it more reasonable to
believe that representatives of these organizations “don't
think for themselves or review the research,
they are lemmings, followers, part of a
herd, not scientists, most are either
ignorant or willfully blind. … or are indeed
sociopaths motivated by power,
prestige and paychecks”
–– or,since there is no legitimate evidence supporting the anti-F–
opinions, a workable alternative is to convince people those who support CWF
can’t be trusted.
k.
FOs Make
Out-Of-context, Irrelevant, Misleading Presentations of Article/Study
Conclusions: Unless one takes the
time to review and understand every claim made by FOs, one will never know what
content has been taken out of context to create a false or misleading claim – it
is wise to consider all ‘evidence’ for anti-F–
claims ‘modified’ in some manner since the overwhelming majority of relevant
experts do not accept the anti-fluoridation interpretations and presentations as
valid.
· As an example, CarryAnne (08-18-2019
08:17 AM) provided an
out of context quote from an article that actually concluded fluoridation was
effective. Specifically CarryAnne
quoted the
2013 European Food Safety Authority review,
Scientific Opinion on Dietary Reference Values for fluoride:
“Fluoride has no known essential function in
human growth and development and no signs of fluoride deficiency have been
identified.”
The rest of the summary was conveniently ignored: “Though fluoride is not essential for tooth
development, exposure to fluoride leads
to incorporation into the hydroxyapatite of the developing tooth enamel and
dentin. The resulting fluorohydroxyapatite is more resistant to acids than
hydroxyapatite. Thus, teeth which contain fluoroapatite are less likely to
develop caries. Apart from
incorporation of fluoride into the dentin and enamel of teeth before eruption,
dietary fluoride exerts an anticaries
effect on erupted teeth through contact with enamel during consumption,
excretion into saliva and uptake into biofilms on teeth. In addition, fluoride
interferes with the metabolism of oral microbial cells, by directly inhibiting,
for example, glycolytic enzymes and cell membrane-associated H+ ATPases in
microbial cells after entry of hydrofluoric acid into their cytoplasm.
(Summary, page 2).
When considering the effectiveness of a
substance for reducing the risk of tooth decay and improving health, it is
irrelevant whether that substance is considered to have an “essential function”
in the context of diet
–– I imagine most rational experts would consider protecting health a very
important, if not essential, function in the context of supporting vs. opposing
CWF.
·
Another CarryAnne example: (09-13-2018 03:44 PM) “Existing data indicate that subsets of the population may be unusually susceptible to the toxic effects of fluoride and its compounds. These populations include the elderly, people with deficiencies of calcium, magnesium, and/or vitamin C, and people with cardiovascular and kidney problems…. Post menopausal women and elderly men in fluoridated communities may also be at risk of fractures.” -
United States Public Health Service Report
(ATSDR TP-91/17, Sec.2.7, April
1993)
In the example above, the quote included everything in the paragraph from the US
Public Health Service review EXCEPT
the last two sentences, which were conveniently scrubbed out – and which
actually support the scientific consensus that fluoridation does not cause
adverse health effects. Here is rest of the quote for appropriate context:
“For most of these populations,
there are very limited data to support or refute increased susceptibility to
fluoride. Additionally, there are no data to suggest that exposure to typical fluoride drinking
water levels would result in adverse effects in these potentially
susceptible populations.” (Page 162-163)
· Note the most of the examples provided above about how anti-fluoridation activists present their arguments to the public demonstrate their complete disregard for a transparent, accurate, presentation of the scientific evidence related to CWF.
8. Bottom Line: If you have read this far, I appreciate your willingness to examine arguments for trusting the overwhelming majority of scientists and health professionals and the scientific consensus over the outlier, anti-fluoridation opinions. I hope I have provided sufficient evidence, without a detailed examination of hundreds of studies, to cast serious doubt on the arguments and tactics of FOs. As previously noted, I began my investigation of the risks and benefits of CWF because of concerns from reading anti-fluoridation arguments. I had, and still have, no predisposition either for or against CWF, and I have absolutely nothing to gain or lose because of my position on CWF. I am simply concerned about the accurate interpretation and representation of scientific evidence, whether it relates to CWF, vaccination, evolution, climate change, and other topics where extremely strong personal beliefs often dictates what someone will believe instead of an impartial evaluation of the relevant body of evidence. During my years of investigation I found no evidence that even strongly suggested CWF didn’t reduce the risk of dental decay (particularly in disadvantaged communities) or that it lowered IQ and/or caused numerous health problems. If I had found such evidence, I would not continue to be a CWF supporter – and I would certainly not try to convince others that support of CWF is an important public health measure that should be supported. There are dozens of factors that can increase or decrease the risk of dental decay. All methods known to increase risk should be minimized and all methods that reduce the risk (including fluoridation) should be implemented.
Respectfully, Randy Johnson, MS

 “Scientists will find the truth because they are committed to finding it,
and they know if they screw up, other scientists will be more than willing to
debunk their shoddy findings. Lone, “one scientist” discoveries are rare. Most
factual conclusions are the product of many individuals and groups checking and
cross-checking each other.”
Dave McMillan
“Scientists will find the truth because they are committed to finding it,
and they know if they screw up, other scientists will be more than willing to
debunk their shoddy findings. Lone, “one scientist” discoveries are rare. Most
factual conclusions are the product of many individuals and groups checking and
cross-checking each other.”
Dave McMillan
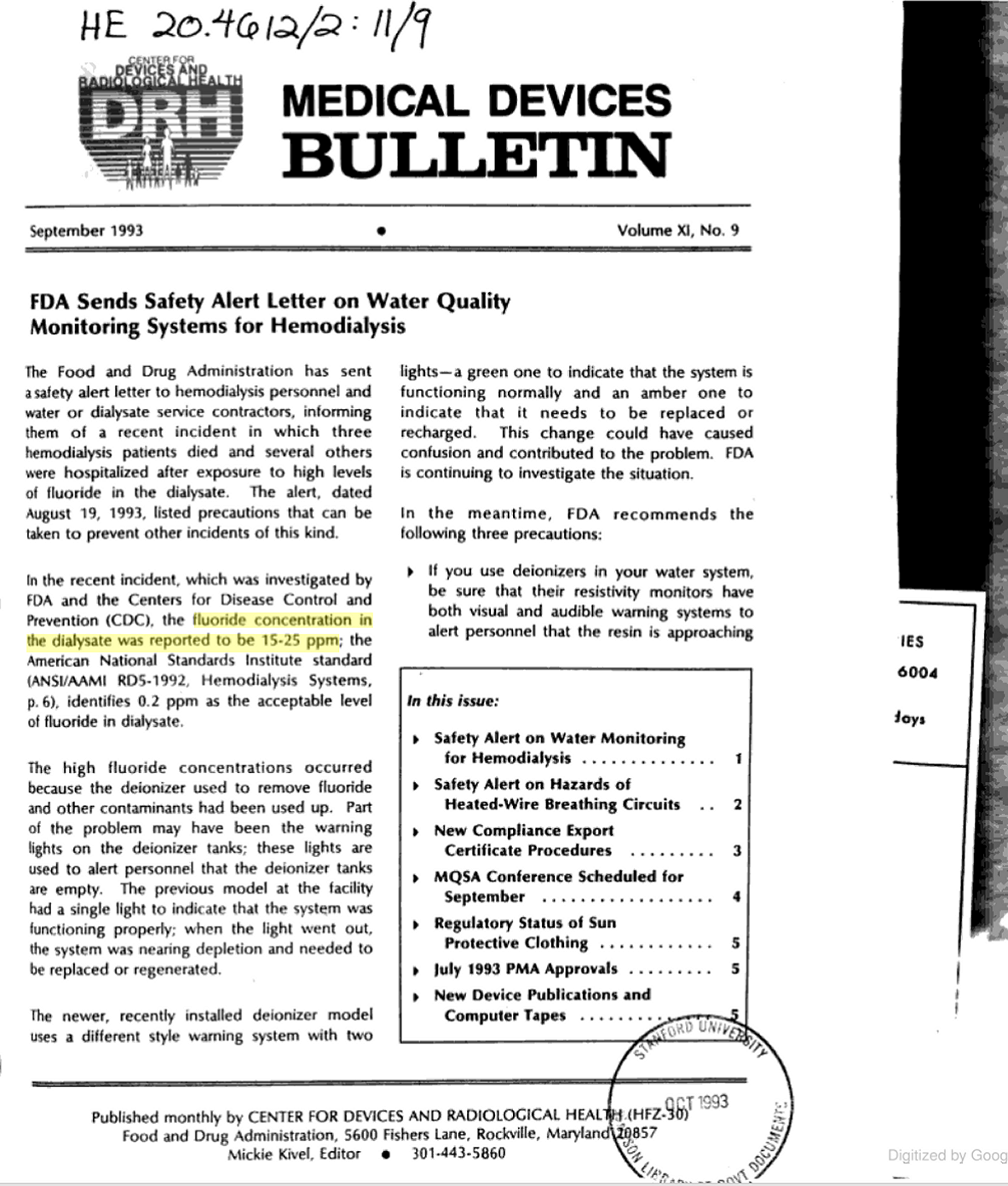{kind=link}